You might also like
- Illumination: "The Established Leader Ee Review"Document6 pagesIllumination: "The Established Leader Ee Review"IVex Brykz Jay Ro60% (5)
- ANEP-25 (Environmental Factors For Surface Ships)Document81 pagesANEP-25 (Environmental Factors For Surface Ships)Bahadır HarmancıNo ratings yet
- MD RAKIBUL ISLAM Update CVDocument2 pagesMD RAKIBUL ISLAM Update CVনীল বেদনাNo ratings yet
- AI in Health CareDocument20 pagesAI in Health CareSebastian ArdilesNo ratings yet
- 3 Virtual Reality in Healthcare: 1.1. Definition of VE and VRDocument30 pages3 Virtual Reality in Healthcare: 1.1. Definition of VE and VRPollo MachoNo ratings yet
- Computers & Graphics: Bernhard Preim, Patrick SaalfeldDocument22 pagesComputers & Graphics: Bernhard Preim, Patrick SaalfeldHasbi MuhammadNo ratings yet
- Complementing Anatomy Education Using Three-Dimensional Anatomy Mobile Software Applications On Tablet ComputersDocument8 pagesComplementing Anatomy Education Using Three-Dimensional Anatomy Mobile Software Applications On Tablet ComputersNizharRismawanNo ratings yet
- Medical Education - Simulation and Virtual RealityDocument2 pagesMedical Education - Simulation and Virtual Realityapi-688059491No ratings yet
- Research ProposalDocument16 pagesResearch Proposalts.kr1020No ratings yet
- Virtual 3D Atlas of A Human Body - Development of An Educational Medical Software ApplicationDocument13 pagesVirtual 3D Atlas of A Human Body - Development of An Educational Medical Software ApplicationRajesh S VNo ratings yet
- ID 441 - Advancements in Manikin TechnologyDocument6 pagesID 441 - Advancements in Manikin TechnologyuviharshNo ratings yet
- 6932-Article Text-54139-3-10-20230925Document8 pages6932-Article Text-54139-3-10-20230925dr.teguhyudhaNo ratings yet
- 1 s2.0 S2095809918301887 MainDocument15 pages1 s2.0 S2095809918301887 MainBudi Utami FahnunNo ratings yet
- Modern Methods Used in The Study of Human AnatomyDocument5 pagesModern Methods Used in The Study of Human AnatomyThe ResercherNo ratings yet
- Anatomy VR 3Document10 pagesAnatomy VR 3lubos.danisovicNo ratings yet
- OverView VirtualRealityinMedicine JVWRDocument37 pagesOverView VirtualRealityinMedicine JVWRHeaven varghese C S C SNo ratings yet
- A Survey On Deep Learning in Medical Image Analysis: Haugeland 1985Document38 pagesA Survey On Deep Learning in Medical Image Analysis: Haugeland 1985Sangat BaikNo ratings yet
- Virtual Reality Article PublishedDocument16 pagesVirtual Reality Article PublishedSonia RodriiguezNo ratings yet
- Ethnography - Guusje Bressers Et Al - 2020Document19 pagesEthnography - Guusje Bressers Et Al - 2020Rucsandra StanNo ratings yet
- Digital Anatomy Applications of Virtual Mixed and Augmented Reality - Jean François Uhl Joaquim Jorge Daniel Simões Lopes Pedro F. CamposDocument388 pagesDigital Anatomy Applications of Virtual Mixed and Augmented Reality - Jean François Uhl Joaquim Jorge Daniel Simões Lopes Pedro F. CamposohundperNo ratings yet
- Anatomy VR 2Document7 pagesAnatomy VR 2lubos.danisovicNo ratings yet
- The Application of 3D Printing in Anatomy EducationDocument4 pagesThe Application of 3D Printing in Anatomy EducationJavier Felipe Gallo BecerraNo ratings yet
- Fourcade 2019Document10 pagesFourcade 2019morganNo ratings yet
- Herron 2016 AugmentedDocument7 pagesHerron 2016 Augmentedfuki nanginamoNo ratings yet
- Virtual Reality in Medical EducationDocument19 pagesVirtual Reality in Medical Educationapi-688059491No ratings yet
- Virtual Reeducation A New Technology: Professeur R. BONIVER O.R.L. Professeur À L'université de LIEGEDocument24 pagesVirtual Reeducation A New Technology: Professeur R. BONIVER O.R.L. Professeur À L'université de LIEGEraymond boniverNo ratings yet
- Microstrip Antennas For Direct Human Skin Placement For Biomedical ApplicationsDocument7 pagesMicrostrip Antennas For Direct Human Skin Placement For Biomedical ApplicationsMai VũNo ratings yet
- Assignment RMDocument11 pagesAssignment RMZaibi's CreationsNo ratings yet
- Human ArgDocument4 pagesHuman ArgSachin ISE-2020-24No ratings yet
- Alinier G. Med Teach. 2007 29Document9 pagesAlinier G. Med Teach. 2007 29Esteban RamosNo ratings yet
- 6Document7 pages6GSL SMART LABNo ratings yet
- Texto 1 RDocument7 pagesTexto 1 ROmid Ernesto Chahuaris ChoqueNo ratings yet
- Scalese2008 Article SimulationTechnologyForSkillsTDocument4 pagesScalese2008 Article SimulationTechnologyForSkillsTAbc DefNo ratings yet
- The Mobile Fitness Coach: Towards Individualized Skill Assessment Using Personalized Mobile DevicesDocument14 pagesThe Mobile Fitness Coach: Towards Individualized Skill Assessment Using Personalized Mobile DevicesLaxman ShresthaNo ratings yet
- Anato PDFDocument6 pagesAnato PDFMaria FGNo ratings yet
- The Effectiveness of Virtual Reality-BasedDocument10 pagesThe Effectiveness of Virtual Reality-Basedapi-688059491No ratings yet
- 1 s2.0 S1361841516300342 MainDocument17 pages1 s2.0 S1361841516300342 Mainzhujin1121No ratings yet
- 10.1002 Ar.b.20069Document6 pages10.1002 Ar.b.20069emnoehNo ratings yet
- A Survey On Deep Learning in Medical Image AnalysiDocument35 pagesA Survey On Deep Learning in Medical Image AnalysiMohamed Ali CHERNINo ratings yet
- Survey On Deep Learning For Medical Imaging: December 2018Document14 pagesSurvey On Deep Learning For Medical Imaging: December 2018Edward Ventura BarrientosNo ratings yet
- Self-Diagnosis With Advanced Hospital Management-IJRASETDocument5 pagesSelf-Diagnosis With Advanced Hospital Management-IJRASETIJRASETPublicationsNo ratings yet
- A Guide To Deep Learning in Healthcare: Nature Medicine January 2019Document7 pagesA Guide To Deep Learning in Healthcare: Nature Medicine January 2019Buster FoxxNo ratings yet
- VR Training in Health Care PDFDocument8 pagesVR Training in Health Care PDFthidayat15No ratings yet
- Ophthalmoscopy Simulation Advances in Training and Practice For Medical Students and Young OphthalmologistsDocument6 pagesOphthalmoscopy Simulation Advances in Training and Practice For Medical Students and Young OphthalmologistsNour hane BiadNo ratings yet
- Maria Paper AdvanceDocument46 pagesMaria Paper AdvanceIDRISS IDRISSNo ratings yet
- 2016 - Utilizing Virtual and Augmented Reality For Educational and Clinical Enhancements in NeurosurgeryDocument4 pages2016 - Utilizing Virtual and Augmented Reality For Educational and Clinical Enhancements in NeurosurgeryTejesh PatelNo ratings yet
- Review of DL in Minimally Invasive SurgeryDocument21 pagesReview of DL in Minimally Invasive SurgeryJoel JacobNo ratings yet
- Anatomia 01 00014Document14 pagesAnatomia 01 00014MaxNo ratings yet
- Icorr17 0168 Fi-1Document7 pagesIcorr17 0168 Fi-1Muhammad ImronNo ratings yet
- 05.succeeding Generation of Augmented Reality TechnolDocument7 pages05.succeeding Generation of Augmented Reality TechnolPreet JainNo ratings yet
- Depp Learning For Medical Image ProcessingDocument57 pagesDepp Learning For Medical Image Processingderricktab44No ratings yet
- A Review of The Use of Virtual Reality Head-Mounted Displays in Education and TrainingDocument15 pagesA Review of The Use of Virtual Reality Head-Mounted Displays in Education and TrainingesrNo ratings yet
- Comprehensive Healthcare Simulation: Improving Healthcare SystemsFrom EverandComprehensive Healthcare Simulation: Improving Healthcare SystemsEllen S. DeutschNo ratings yet
- 10 1108 - Dta 08 2021 0210Document14 pages10 1108 - Dta 08 2021 0210nasiruddinNo ratings yet
- Task 8Document20 pagesTask 8api-688059491No ratings yet
- Simulation in NursingDocument12 pagesSimulation in Nursingkateypark1485No ratings yet
- Kruger 2021 BJOT In-Hand Manipulation Assessments Scoping ReviewDocument17 pagesKruger 2021 BJOT In-Hand Manipulation Assessments Scoping ReviewAnnelize KrugerNo ratings yet
- 1 s2.0 S2414644720300208 MainDocument4 pages1 s2.0 S2414644720300208 MainWindu KumaraNo ratings yet
- Mos - Metaverse in Healthcare 1Document15 pagesMos - Metaverse in Healthcare 1priyanka srivastavaNo ratings yet
- Current Limitations Into The Application of Virtual Reality To Mental Health ResearchDocument4 pagesCurrent Limitations Into The Application of Virtual Reality To Mental Health Researchclyde.machado3225No ratings yet
- 2019 Book BrainAndHumanBodyModeling PDFDocument398 pages2019 Book BrainAndHumanBodyModeling PDFCosme MejiaNo ratings yet
- Litrature ReviewDocument4 pagesLitrature ReviewWondwosen YimerNo ratings yet
- Mapping Study of Computer Vision Tools Applied ToDocument6 pagesMapping Study of Computer Vision Tools Applied ToTHEGARYANQUINo ratings yet
- Paranormal Activity 3Document5 pagesParanormal Activity 3alexNo ratings yet
- AULA 13 - RespondidoDocument4 pagesAULA 13 - RespondidoRanyelle WanessaNo ratings yet
- Sand Reclamation - Standard Devices: Shake Out MachinesDocument2 pagesSand Reclamation - Standard Devices: Shake Out MachinesKaarthicNatarajanNo ratings yet
- Role of Technology in AdvertisementtDocument29 pagesRole of Technology in AdvertisementtShalini ChatterjeeNo ratings yet
- Cummins ECM Reference NotesDocument11 pagesCummins ECM Reference NotesjuanNo ratings yet
- Hydraulic Cartridge SystemsDocument14 pagesHydraulic Cartridge SystemsJas SumNo ratings yet
- KOSO-KI Vector-Disk Stack BrochureDocument11 pagesKOSO-KI Vector-Disk Stack Brochureनिखिल बायवारNo ratings yet
- Etap - Relay CoordinationDocument311 pagesEtap - Relay CoordinationManohar Potnuru100% (1)
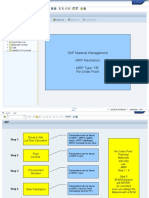
- SAP Material Management MRP Mechanics MRP Type "VB" Re-Order PointDocument15 pagesSAP Material Management MRP Mechanics MRP Type "VB" Re-Order PointmohhitNo ratings yet
- IPCR Part 2 2017Document4 pagesIPCR Part 2 2017RommelNo ratings yet
- Ad Agency SynopsisDocument19 pagesAd Agency SynopsisRaj BangaloreNo ratings yet
- Electrical Load For Indoor UnitsDocument2 pagesElectrical Load For Indoor UnitsMD BILAL ASLAMNo ratings yet
- NessusDocument23 pagesNessusShivaprakash TimmapurNo ratings yet
- ORF Issue Brief 309 SpaceLawDocument12 pagesORF Issue Brief 309 SpaceLawNitish KumarNo ratings yet
- Lab Manual No 13Document3 pagesLab Manual No 13Hammad JawadNo ratings yet
- Step-By-Step Guide - Sensors Alarms1Document14 pagesStep-By-Step Guide - Sensors Alarms1Andy_kokoNo ratings yet
- How To Use MySQL With ErlangDocument2 pagesHow To Use MySQL With ErlangarthurbulivaNo ratings yet
- Contactor HassDocument1 pageContactor Hassecaldera10No ratings yet
- Xid-2025857 1Document6 pagesXid-2025857 1Thanh NguyenNo ratings yet
- Operation and Maintenance Manual: Mux-2200E Integrated Service MultiplexerDocument82 pagesOperation and Maintenance Manual: Mux-2200E Integrated Service Multiplexerlee.tetleie1675No ratings yet
- Abu Dhabi Certification Scheme For Assistant EngineerDocument12 pagesAbu Dhabi Certification Scheme For Assistant EngineersureshNo ratings yet
- Instalación Sensor RPM TurboDocument13 pagesInstalación Sensor RPM TurboLuis Herrera MarinNo ratings yet
- D-1967 (Clean) Quilting Machine ManualDocument33 pagesD-1967 (Clean) Quilting Machine Manualvalter craccoNo ratings yet
- GEK 116403 Ge File. Performance TestsDocument54 pagesGEK 116403 Ge File. Performance TestsSulaiman JafferyNo ratings yet
- Leaflet US5Ge ProtectedDocument3 pagesLeaflet US5Ge Protectedquochung0606No ratings yet
- Homework 1&2 Report EE440Document19 pagesHomework 1&2 Report EE440Võ Hoàng Chương100% (1)
- E3D2 1version-1Document12 pagesE3D2 1version-1Nikolay NachevNo ratings yet