You might also like
- Electrical Stimulation: Prepared By: Floriza P. de LeonDocument49 pagesElectrical Stimulation: Prepared By: Floriza P. de LeonFloriza de Leon75% (4)
- Proposed New RO Water Fencing MethodDocument14 pagesProposed New RO Water Fencing MethodLuwalhati Tomilas100% (6)
- Cleftlipandpalate 111008125422 Phpapp02Document81 pagesCleftlipandpalate 111008125422 Phpapp02samira fatimaNo ratings yet
- Stroke Rehabilitation: School of Medicine Brawijaya UniversityDocument47 pagesStroke Rehabilitation: School of Medicine Brawijaya UniversityAldiola PerdanaNo ratings yet
- NATA 2015 Presentation - Dan Houglum PDFDocument77 pagesNATA 2015 Presentation - Dan Houglum PDFRaunaq Salat100% (1)
- KV Barrackpore Physical Education Project History of CricketDocument31 pagesKV Barrackpore Physical Education Project History of CricketRamesh Chand100% (1)
- Teach Yourself Pelvis and PerineumDocument23 pagesTeach Yourself Pelvis and PerineumHarun Mohamed100% (1)
- Physical Therapy Clinical ManagementDocument24 pagesPhysical Therapy Clinical ManagementClaudia MicuNo ratings yet
- De Quervain SyndromeDocument5 pagesDe Quervain SyndromePaula ZorziNo ratings yet
- Dragon Keeper Chap 21-24questionsDocument9 pagesDragon Keeper Chap 21-24questionsapi-2328088250% (2)
- Safety in Welding & CuttingDocument19 pagesSafety in Welding & CuttingPritesh Ramesh Bare100% (1)
- CPDocument85 pagesCPSudhir MishraNo ratings yet
- Worksafe Manual HandlingDocument18 pagesWorksafe Manual HandlingtahseenhassantirmiziNo ratings yet
- Special Tests For WristDocument13 pagesSpecial Tests For WristSaif Ahmed LariNo ratings yet
- Journal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDDocument9 pagesJournal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDWinda FRNo ratings yet
- Gpu 400 3 Phase and Maintenance ManualDocument116 pagesGpu 400 3 Phase and Maintenance ManualLe SonNo ratings yet
- Pott's SpineDocument47 pagesPott's Spinesigarun67% (3)
- Fractures in the Elderly: Types, Causes and TreatmentsDocument27 pagesFractures in the Elderly: Types, Causes and TreatmentshazelelNo ratings yet
- NCM103A W3 Range of Motion Module - 1774822568Document9 pagesNCM103A W3 Range of Motion Module - 1774822568Esvinch EsvinchNo ratings yet
- Maceira EDocument21 pagesMaceira EDewidewidewi Madridista Part II100% (1)
- Acl Reconstruction ProtocolDocument8 pagesAcl Reconstruction ProtocolMestereaga AlinNo ratings yet
- Lumbar PunctureDocument23 pagesLumbar Puncturemamoon100% (2)
- Road Traffic Safety (RTS) Management System ISO 39001:2012Document30 pagesRoad Traffic Safety (RTS) Management System ISO 39001:2012Subhash Mukherjee80% (5)
- After Surgery Rehabilitation Program MPFL ReconstructionDocument12 pagesAfter Surgery Rehabilitation Program MPFL ReconstructionNedelcu NicolaeNo ratings yet
- Effectiveness of Cupping Therapy Versus Myofascial Release (MFR) in Reducing Gastrocnemius Muscle Tightness in High Heels Users - A Comparative StudyDocument6 pagesEffectiveness of Cupping Therapy Versus Myofascial Release (MFR) in Reducing Gastrocnemius Muscle Tightness in High Heels Users - A Comparative StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Slide Bells PalsyDocument74 pagesSlide Bells PalsyIrithca Jayanty TengkerNo ratings yet
- Pott's DiseaseDocument34 pagesPott's DiseaseNicole Marin-ChingNo ratings yet
- Klippel Trenaunay SyndromeDocument15 pagesKlippel Trenaunay SyndromeamsirlimbongNo ratings yet
- NCP Impaired Skin IntegrityDocument2 pagesNCP Impaired Skin IntegrityEden Marie Francisco100% (2)
- Brachial Plexus Injury in Neonates: Anatomy, Pathogenesis, Clinical Manifestations, Diagnosis and ManagementDocument31 pagesBrachial Plexus Injury in Neonates: Anatomy, Pathogenesis, Clinical Manifestations, Diagnosis and ManagementRahma WulanNo ratings yet
- Referral of Diagnosis and Management of Erb-Duchenne PalsyDocument22 pagesReferral of Diagnosis and Management of Erb-Duchenne PalsyAshielaNo ratings yet
- Erb Duchenne Palsy PresentationDocument19 pagesErb Duchenne Palsy PresentationAshielaNo ratings yet
- Transcutaneous Electrical Nerve Stimulation (TENS)Document52 pagesTranscutaneous Electrical Nerve Stimulation (TENS)nobodyNo ratings yet
- BPI Okt - JunaidiDocument28 pagesBPI Okt - Junaidiwahyu_sitaNo ratings yet
- Faktor Risiko Gizi Buruk Pada Balita Di Kabupaten Donggala Provinsi Sulawesi TengahDocument10 pagesFaktor Risiko Gizi Buruk Pada Balita Di Kabupaten Donggala Provinsi Sulawesi TengahEny AnggaraeniNo ratings yet
- Presentation Brachial Plexus Injuries in PeadsDocument30 pagesPresentation Brachial Plexus Injuries in Peadskashmala afzalNo ratings yet
- Theraex For IKFRDocument130 pagesTheraex For IKFRsingle_ladyNo ratings yet
- Arthrogryposis Congenital ContractureDocument32 pagesArthrogryposis Congenital ContractureMayesa Akiro100% (1)
- Video Based Observational Gait AnalysisDocument77 pagesVideo Based Observational Gait AnalysisRashidkpvldNo ratings yet
- Anatomi dan Kinesiologi Tangan (1Document66 pagesAnatomi dan Kinesiologi Tangan (1Ika Ayu ParamitaNo ratings yet
- Brachial Plexus InjuryDocument21 pagesBrachial Plexus InjurySemi IqbalNo ratings yet
- Case Report: Osteoarthritis: Mutiara Riahna Sitepu 030.12.179 Pembimbing Dr. T. Nurrobi, SP - OT (K) HandDocument50 pagesCase Report: Osteoarthritis: Mutiara Riahna Sitepu 030.12.179 Pembimbing Dr. T. Nurrobi, SP - OT (K) Handmutiara sitepuNo ratings yet
- Rehabilitasi Pasca CABGDocument23 pagesRehabilitasi Pasca CABGPaulina WowilingNo ratings yet
- Painful Hemiplegic ShoulderDocument53 pagesPainful Hemiplegic ShoulderpipitNo ratings yet
- 2012 Rehabilitation of Brachial Plexus Injuries in Adults and ChildrenDocument24 pages2012 Rehabilitation of Brachial Plexus Injuries in Adults and ChildrenchayankkuNo ratings yet
- Tinpus HNPDocument34 pagesTinpus HNPDimas JanuarNo ratings yet
- CV Dr Tirza Z Tamin Rehabilitation ExpertDocument71 pagesCV Dr Tirza Z Tamin Rehabilitation ExpertAnastasia WibiantoNo ratings yet
- Exercise Metabolism, Carbohydrates and LipidsDocument39 pagesExercise Metabolism, Carbohydrates and LipidsMohdSyamRoslanNo ratings yet
- Developmental Dysplasia of The HipDocument20 pagesDevelopmental Dysplasia of The Hipdanyky19No ratings yet
- Orthopaedic Textbook Explains Blount's DiseaseDocument17 pagesOrthopaedic Textbook Explains Blount's DiseaseFadzhil AmranNo ratings yet
- Proprioceptive Neuromuscular Facilitation (PNF) Stretching Techniques Hold-Relax HR ALLDocument8 pagesProprioceptive Neuromuscular Facilitation (PNF) Stretching Techniques Hold-Relax HR ALLKiné Therapeut-manuelle Masseur GabiNo ratings yet
- Eng Transtibial PDFDocument52 pagesEng Transtibial PDFRudi NugrahaNo ratings yet
- Upper Cervical Injuries Diagnosis and TreatmentDocument36 pagesUpper Cervical Injuries Diagnosis and TreatmentesterhsNo ratings yet
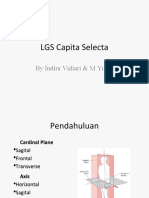
- LGS Capita Selecta: by Indira Vidiari & M YusufDocument30 pagesLGS Capita Selecta: by Indira Vidiari & M YusufniekoNo ratings yet
- DDH - PFDocument34 pagesDDH - PFAnnisa Oktoviani MursidaNo ratings yet
- Developmental Coordination DisorderDocument7 pagesDevelopmental Coordination DisorderQina Nugroho, pts.No ratings yet
- Nur Rachmat Lubis: Divisi Orthopaedi Dept Bedah FK UNSRI/ RS Dr. M. Hoesin PalembangDocument38 pagesNur Rachmat Lubis: Divisi Orthopaedi Dept Bedah FK UNSRI/ RS Dr. M. Hoesin Palembangsoleha09la solehaNo ratings yet
- Treating Patients With Hemiplegic Shoulder Pain PDFDocument12 pagesTreating Patients With Hemiplegic Shoulder Pain PDFasdar fajrinNo ratings yet
- Hip Replacement GuideDocument28 pagesHip Replacement GuideZulaika NaisNo ratings yet
- The Pathophysiology of SpasticityDocument18 pagesThe Pathophysiology of SpasticityjpwchardonNo ratings yet
- Workers at Kampung Sepatu, Kelurahan Miji, Kecamatan Prajurit Kulon, Kota Mojokerto)Document8 pagesWorkers at Kampung Sepatu, Kelurahan Miji, Kecamatan Prajurit Kulon, Kota Mojokerto)irvanagheNo ratings yet
- Effect of Long Distance Cycling on Ulnar NerveDocument30 pagesEffect of Long Distance Cycling on Ulnar NervesherysheryyNo ratings yet
- Hallux Valgus: Sartika Pradhipta Cahya 20204010030Document18 pagesHallux Valgus: Sartika Pradhipta Cahya 20204010030sartika cahyaNo ratings yet
- 11.sitoskeleton Dan Pergerakan Sel-Dr - IsraDocument40 pages11.sitoskeleton Dan Pergerakan Sel-Dr - IsraTa RaNo ratings yet
- Spondylitis TBDocument33 pagesSpondylitis TBYohana KoliNo ratings yet
- Kinesiology ElbowDocument53 pagesKinesiology Elbowsingle_ladyNo ratings yet
- Growth Plate InjuriesDocument41 pagesGrowth Plate Injurieskosmynin86No ratings yet
- PCL's Avulsion FractureDocument22 pagesPCL's Avulsion FractureNey da OnneyNo ratings yet
- Askep Atresia EsophagusDocument18 pagesAskep Atresia EsophagusKhoLisoh Sae Anugrah100% (1)
- Acl Reconstruction ProtocolDocument8 pagesAcl Reconstruction ProtocolFahd AbdelazimNo ratings yet
- Mat ActivitiesDocument2 pagesMat ActivitiesAtul SrivastavaNo ratings yet
- Temporo-Mandibular Joint Complex Exercise SuggestionsDocument9 pagesTemporo-Mandibular Joint Complex Exercise SuggestionsClaudia LeperaNo ratings yet
- LCPDDocument7 pagesLCPDakoismeNo ratings yet
- DelhiDocument8 pagesDelhiEinstein JeromeNo ratings yet
- ConferenceDocument9 pagesConferenceEinstein JeromeNo ratings yet
- PT PointsDocument1 pagePT PointsEinstein JeromeNo ratings yet
- Pediatric Assessment NSCDocument63 pagesPediatric Assessment NSCEinstein JeromeNo ratings yet
- Functional Anatomy of The Upper ExtremityDocument46 pagesFunctional Anatomy of The Upper ExtremityEinstein JeromeNo ratings yet
- The Skeletal System: By: Jasper C. Pilongo, M.DDocument110 pagesThe Skeletal System: By: Jasper C. Pilongo, M.Dash_zordickNo ratings yet
- Bladder TraumaDocument13 pagesBladder TraumaBernardNo ratings yet
- Nevada Slip and Fall Attorneys | Benson & BinghamDocument10 pagesNevada Slip and Fall Attorneys | Benson & BinghamBenson & Bingham Accident Injury Lawyers, LLCNo ratings yet
- Physical Education and Health 11: Learning Activity Sheet (Week 5-6) Personal Safety Background InformationDocument4 pagesPhysical Education and Health 11: Learning Activity Sheet (Week 5-6) Personal Safety Background InformationRheena-Ann Dupale PadillaNo ratings yet
- McGill Pain QuestionnaireDocument17 pagesMcGill Pain Questionnaireramanrajesh83No ratings yet
- The Laws of The Earliest English KingsDocument276 pagesThe Laws of The Earliest English KingsOopsNo ratings yet
- Surface Anatomy of The Upper LimbDocument3 pagesSurface Anatomy of The Upper LimbIrvin JoshuaNo ratings yet
- Posterior Ankle Impingement - Soft Tissue - Rayner & Smale PDFDocument3 pagesPosterior Ankle Impingement - Soft Tissue - Rayner & Smale PDFItai IzhakNo ratings yet
- Forensic BallisticDocument12 pagesForensic BallisticYash GuptaNo ratings yet
- Abdominal Incision TypesDocument36 pagesAbdominal Incision TypesMiftah AjiNo ratings yet
- Health Week 4 - 3rd QuarterDocument5 pagesHealth Week 4 - 3rd QuarterNoemelyn VecinaNo ratings yet
- Mpu Exercise1Document20 pagesMpu Exercise1PrimadonnaNganNo ratings yet
- Offensive Play: How Different Are Dogfighting and Football?Document10 pagesOffensive Play: How Different Are Dogfighting and Football?milandeepNo ratings yet
- Adaptive Pe Lesson PlanDocument3 pagesAdaptive Pe Lesson Planapi-302063651No ratings yet
- 90213-1016DED F-Zeroing Motor ReplaceDocument55 pages90213-1016DED F-Zeroing Motor ReplaceIsaac CarmonaNo ratings yet
- Traumaplant DR Alon Doctor Internet 1267604597333Document3 pagesTraumaplant DR Alon Doctor Internet 1267604597333Salvator2000No ratings yet
- Classification of Age-Related CataractDocument16 pagesClassification of Age-Related CataractShari' Si WahyuNo ratings yet