You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Leactur IV - Employee Testing & SelectionDocument32 pagesLeactur IV - Employee Testing & SelectionMEHWISH MAHMOOD100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Res12 Module 2Document20 pagesRes12 Module 2Yanchen KylaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Tugas Sia 1 Sept 2Document19 pagesTugas Sia 1 Sept 2Fadli Arif SetiawanNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Corresponding Author:: Finea@uci - EduDocument55 pagesCorresponding Author:: Finea@uci - EdualainremyNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Mayer Et Al-2007 PDFDocument11 pagesMayer Et Al-2007 PDFKarsten HerrNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Initial Development of An Inventory To Assess Stress and Health RiskDocument8 pagesInitial Development of An Inventory To Assess Stress and Health RiskMayra Gómez LugoNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- MODULE 2 HandoutDocument25 pagesMODULE 2 HandoutLady Edzelle AliadoNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
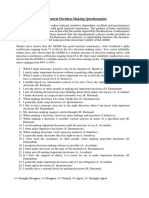
- GDMS FinalDocument1 pageGDMS FinalJoysri RoyNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Ahmad 2014 - The Perceived Impact of JIT Implementation On Firms Financial Growth PerformanceDocument13 pagesAhmad 2014 - The Perceived Impact of JIT Implementation On Firms Financial Growth Performanceapostolos thomasNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Validation of The Constitution in Chinese MedicineDocument15 pagesValidation of The Constitution in Chinese MedicineBắp QuyênNo ratings yet
- Validation of The Standardized Version of RQLQ Juniper1999Document6 pagesValidation of The Standardized Version of RQLQ Juniper1999IchsanNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Standardized Tests and The Diagnosis of Speech Sound DisordersDocument9 pagesStandardized Tests and The Diagnosis of Speech Sound Disordersanyush babayanNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Evaluation of The New York Posture Rating Chart For Assessing Changes in Postural Alignment in A Garment StudyDocument17 pagesEvaluation of The New York Posture Rating Chart For Assessing Changes in Postural Alignment in A Garment StudyKOTA DAMANSARA HEALTHY SPINE CARENo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Humphrey Field AnalyzerTMDocument44 pagesHumphrey Field AnalyzerTMsayumiholic890% (1)
- Therapist Nonverbal Behavior and Perceptions of Empathy, Alliance, and Treatment CredibilityDocument8 pagesTherapist Nonverbal Behavior and Perceptions of Empathy, Alliance, and Treatment Credibilityc.limaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- E-Book Measuring EWOMDocument385 pagesE-Book Measuring EWOMToni Ahmad SubektiNo ratings yet
- Language Testing: The Testing of Listening Comprehension: An Introspective Study1Document26 pagesLanguage Testing: The Testing of Listening Comprehension: An Introspective Study1Dini HaryantiNo ratings yet
- OBE Syllabus Language and Lit AssessmentDocument13 pagesOBE Syllabus Language and Lit AssessmentJoefryQuanicoBarcebalNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Effect of Internal Control, Human Resources Competency, and Use of Information Technology On Quality of Financial Statement With Organizational Commitment As Intervening VariablesDocument8 pagesThe Effect of Internal Control, Human Resources Competency, and Use of Information Technology On Quality of Financial Statement With Organizational Commitment As Intervening VariablesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Batangas State University: - 7. "Camille Is Hungry So She Ate in Her Favorite Restaurant."Document5 pagesBatangas State University: - 7. "Camille Is Hungry So She Ate in Her Favorite Restaurant."Christle PMDNo ratings yet
- Panas-Gen About: This Scale Is A Self-Report Measure of Affect. Items: 20Document2 pagesPanas-Gen About: This Scale Is A Self-Report Measure of Affect. Items: 20InsiyaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Comprehensive Material For Measurement and EvaluationDocument54 pagesComprehensive Material For Measurement and EvaluationMary ChildNo ratings yet
- Self-Efficacy and Work Readiness Among Vocational High School StudentsDocument5 pagesSelf-Efficacy and Work Readiness Among Vocational High School StudentsJournal of Education and LearningNo ratings yet
- Lesson Plan in English 10Document7 pagesLesson Plan in English 10IrishJaneDeJesusNo ratings yet
- Psychology ScaleDocument15 pagesPsychology ScaleAmisha MakwanaNo ratings yet
- A Systematic Meta-Review of Measures of Classroom Management in School SettingsDocument32 pagesA Systematic Meta-Review of Measures of Classroom Management in School SettingsRasec OdacremNo ratings yet
- Psychological Assessment - Reliability & ValidityDocument56 pagesPsychological Assessment - Reliability & ValidityAlyNo ratings yet
- Using Routine Comparative Data To Assess The Quality of Health Care: Understanding and Avoiding Common PitfallsDocument7 pagesUsing Routine Comparative Data To Assess The Quality of Health Care: Understanding and Avoiding Common Pitfallsujangketul62No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- 222 ClassX Psychology English Part1Document243 pages222 ClassX Psychology English Part1Sundeep YadavNo ratings yet
- The Korean Version of The Fugl-Meyer AssesmentDocument16 pagesThe Korean Version of The Fugl-Meyer AssesmentEkaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)