You might also like
- Nursing Care Plan for Suicidal PatientDocument4 pagesNursing Care Plan for Suicidal PatientJennifer ArdeNo ratings yet
- Case NCP MelbaDocument2 pagesCase NCP MelbabambheesyeoboNo ratings yet
- Nursing Care Plan Distrubed Sleeping PatternDocument2 pagesNursing Care Plan Distrubed Sleeping Patternferrerjohnoliver86% (59)
- Nursing Care PlanDocument2 pagesNursing Care Plankehyrie100% (2)
- Nursing Care Plan - Activity IntoleranceDocument1 pageNursing Care Plan - Activity IntoleranceLei Ortega67% (9)
- Nursing Care Plan: Angeles University Foundation College of NursingDocument4 pagesNursing Care Plan: Angeles University Foundation College of NursingGerna Anne Salenga CabilingNo ratings yet
- Impaired Physical MobilityDocument1 pageImpaired Physical MobilityAnthony jesusNo ratings yet
- NCP MS DbiDocument2 pagesNCP MS DbiSj EclipseNo ratings yet
- Evolve. Adapt. Overcome. CEFI is now readyDocument8 pagesEvolve. Adapt. Overcome. CEFI is now readyKarl Symon AmperNo ratings yet
- Nursing Care Plan For Post Thyroidectomy and CholecystectomyDocument9 pagesNursing Care Plan For Post Thyroidectomy and Cholecystectomyirish m magracia100% (7)
- Professional Development CMDocument10 pagesProfessional Development CMapi-707173744No ratings yet
- Nursing Care Plan - D & CDocument2 pagesNursing Care Plan - D & Cderic89% (18)
- Nursing Care Plan-PrenatalDocument2 pagesNursing Care Plan-Prenatalbeayap81% (31)
- NCPDocument3 pagesNCPTweenie DalumpinesNo ratings yet
- Care Plan On Acute Transient Psychiatric Disorder 2Document4 pagesCare Plan On Acute Transient Psychiatric Disorder 2Divya ThomasNo ratings yet
- Disturbed SleepDocument1 pageDisturbed Sleepmawel100% (1)
- Schizophrenia NCPDocument4 pagesSchizophrenia NCPDen-rashier M. Jamsuri100% (1)
- NURSING CARE PLAN-Impired Physical MobilityDocument5 pagesNURSING CARE PLAN-Impired Physical MobilityKathleen Leana Viray JeanjaquetNo ratings yet
- Nursing Care Plan: Disturbed Sleeping Pattern Assessment Nursing Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument1 pageNursing Care Plan: Disturbed Sleeping Pattern Assessment Nursing Diagnosis Planning Intervention Rationale Evaluation SubjectiveKryza CastilloNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanNeza AgdalesNo ratings yet
- Coping with body image changes after burnsDocument2 pagesCoping with body image changes after burnspaopao14344No ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanAnonymousTargetNo ratings yet
- Nursing Care Plan for FatigueDocument8 pagesNursing Care Plan for FatigueChad Smith100% (1)
- Transcultural NSG ActDocument5 pagesTranscultural NSG ActDerick Nyl PascualNo ratings yet
- Bipo Care PlanDocument5 pagesBipo Care PlanDivya ThomasNo ratings yet
- Self-Care Deficit R/T Cerebrovascular Accident As Evidenced by Hemiplegia / Poor Personal HygieneDocument1 pageSelf-Care Deficit R/T Cerebrovascular Accident As Evidenced by Hemiplegia / Poor Personal HygieneScarlet PachecoNo ratings yet
- NCP Cva Impaired Physical MobilityDocument2 pagesNCP Cva Impaired Physical Mobilityexcel2112180% (5)
- AppendicitisDocument2 pagesAppendicitisjustinekaye diongsonNo ratings yet
- 2FINAL - Shape Module 4Document110 pages2FINAL - Shape Module 4Rodel CamposoNo ratings yet
- NCP FormatDocument1 pageNCP FormatVhince Norben PiscoNo ratings yet
- NCP (Final) - BipolarDocument6 pagesNCP (Final) - BipolarBel CortezNo ratings yet
- MA OD PPT 1 IntroDocument15 pagesMA OD PPT 1 Introyogesh.kamathNo ratings yet
- Nursing Care Plan for a Client with Ineffective Breathing PatternDocument3 pagesNursing Care Plan for a Client with Ineffective Breathing PatternPrincess Faniega SugatonNo ratings yet
- 11.3 NCP Activity IntoleranceDocument2 pages11.3 NCP Activity IntoleranceJessa AdenigNo ratings yet
- NCP Acitivity IntoleranceDocument3 pagesNCP Acitivity IntolerancegizelleNo ratings yet
- NCP Psych RotationDocument3 pagesNCP Psych RotationFrancis Alfred EscaranNo ratings yet
- NCP and Fdar.Document4 pagesNCP and Fdar.Ralph Laurent De DiosNo ratings yet
- Nursing Care Plan: Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan: Diagnosis Planning Intervention Rationale EvaluationzjaneNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument5 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationgianinaemilleNo ratings yet
- NCP - CopdDocument3 pagesNCP - CopdhystericoNo ratings yet
- Assessment, diagnosis, planning, intervention, and evaluation for Parkinson's patientDocument2 pagesAssessment, diagnosis, planning, intervention, and evaluation for Parkinson's patientBenjie DimayacyacNo ratings yet
- 3 NCP AsthmaDocument6 pages3 NCP AsthmajaninenicoleNo ratings yet
- Assessing ADL CapabilitiesDocument3 pagesAssessing ADL Capabilitiesnor ain b. odingNo ratings yet
- High Ex: - Score Suggests Perience Diffi I Persons S, AdaDocument5 pagesHigh Ex: - Score Suggests Perience Diffi I Persons S, Adapaska chinnappanNo ratings yet
- Skills Checklist - Changing An Unoccupied BedDocument5 pagesSkills Checklist - Changing An Unoccupied BedRonzie EstrellaNo ratings yet
- Assessing and Treating Nutritional ImbalanceDocument1 pageAssessing and Treating Nutritional ImbalanceakhixzNo ratings yet
- Kitchen Risk Assessment Template TitleDocument3 pagesKitchen Risk Assessment Template TitleShah Jahan75% (4)
- Nursing Care Plan IIDocument4 pagesNursing Care Plan IIHarlene Joyce ReyNo ratings yet
- AssessmentDocument2 pagesAssessmentlopezlarisseNo ratings yet
- Lapitan NCP MyelomeningoceleDocument4 pagesLapitan NCP MyelomeningoceleRea LapitanNo ratings yet
- NCP Kuya TedDocument3 pagesNCP Kuya TedBenjie DimayacyacNo ratings yet
- NpiDocument9 pagesNpiBernardNo ratings yet
- Nursing Care Plan: Phinma University of IloiloDocument4 pagesNursing Care Plan: Phinma University of IloiloLestly Mae Tedios MongayaNo ratings yet
- NCP Self Care DeficitDocument2 pagesNCP Self Care DeficitBARRISTERFLOWERSEAURCHIN6No ratings yet
- Western Mindanao State University College of Nursing Fundamentals in Nursing Practice (Lecture) Course Output (Final Term)Document3 pagesWestern Mindanao State University College of Nursing Fundamentals in Nursing Practice (Lecture) Course Output (Final Term)Reann LeeNo ratings yet
- NCP (Gonzales) Mar 29 - Ventura PDFDocument3 pagesNCP (Gonzales) Mar 29 - Ventura PDFJian VenturaNo ratings yet
- Breastfeeding HTPDocument2 pagesBreastfeeding HTPlyn valerieNo ratings yet
- Acute Glomerulonephritis (AGN) OverviewDocument4 pagesAcute Glomerulonephritis (AGN) OverviewJohnhineNo ratings yet
- Ulcerative Colitis Treatment OptionsDocument5 pagesUlcerative Colitis Treatment OptionsJohnhineNo ratings yet
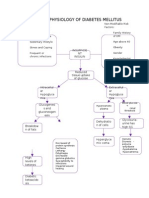
- Pathophysiology of Diabetes MellitusDocument8 pagesPathophysiology of Diabetes MellitusYaniNo ratings yet
- RizalDocument3 pagesRizalJohnhineNo ratings yet
- NR Research 1Document6 pagesNR Research 1JohnhineNo ratings yet
- Pop ObDocument1 pagePop ObJohnhineNo ratings yet
- Journal 1Document1 pageJournal 1JohnhineNo ratings yet
- Ventilator-Associated Pneumonia - Risk Factors & Prevention (Beth Augustyn)Document8 pagesVentilator-Associated Pneumonia - Risk Factors & Prevention (Beth Augustyn)ariepitonoNo ratings yet
- First Aid and CPR Training GuideDocument73 pagesFirst Aid and CPR Training GuidechimaraiykeNo ratings yet
- J-CAPS-02 (SC+MATHS) Class X (1st To 7th May 2020) by AAKASH InstituteDocument5 pagesJ-CAPS-02 (SC+MATHS) Class X (1st To 7th May 2020) by AAKASH Institutemuscularindian0% (1)
- Zoology Finals ReviewerDocument18 pagesZoology Finals ReviewerZian Lei MienNo ratings yet
- CKD NCPDocument4 pagesCKD NCPArlene Macatangay100% (1)
- FU-M2-CU6 LEC Planning Phase-Towards Goals and Outcomes.Document6 pagesFU-M2-CU6 LEC Planning Phase-Towards Goals and Outcomes.Shiro KagomeNo ratings yet
- DLP (Boyle's Law)Document6 pagesDLP (Boyle's Law)Lern JergiNo ratings yet
- Bronchitis PathophysiologyDocument23 pagesBronchitis PathophysiologyRama Setya Bagaskara100% (2)
- Assisting in Tracheostomy and Its Immediate CareDocument13 pagesAssisting in Tracheostomy and Its Immediate CareAnusha VergheseNo ratings yet
- Addis Ababa University Faculty of Medicine Difficult Airway ManagementDocument54 pagesAddis Ababa University Faculty of Medicine Difficult Airway ManagementagatakassaNo ratings yet
- Why Measure Blood Gases A Threepart Introduction For The Novice Part 3Document9 pagesWhy Measure Blood Gases A Threepart Introduction For The Novice Part 3Tibi TibiNo ratings yet
- IDA and AsthmaDocument5 pagesIDA and AsthmacatherineNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument8 pagesChronic Obstructive Pulmonary DiseaseYessamin Paith RoderosNo ratings yet
- Respiratory System SummaryDocument3 pagesRespiratory System Summaryapi-276805445No ratings yet
- Potassium Persulfate InformationDocument3 pagesPotassium Persulfate InformationmeimeiliuNo ratings yet
- Insights: Reducing Transmission of Sars-Cov-2Document4 pagesInsights: Reducing Transmission of Sars-Cov-2epraetorianNo ratings yet
- Bronchipret Patient BrochureDocument5 pagesBronchipret Patient BrochurePetq PetkovaNo ratings yet
- Grade 9 Science LM Complete DraftDocument105 pagesGrade 9 Science LM Complete DraftJerimiah Miranda74% (31)
- Airofit PRO Quick GuideDocument29 pagesAirofit PRO Quick GuideDracones Di Paolo DragoniNo ratings yet
- PARAQUAT POISIONING 3rd Block Imed COMPLIEDDocument15 pagesPARAQUAT POISIONING 3rd Block Imed COMPLIEDMohil PratapNo ratings yet
- Care of Clients with Problems in OxygenationDocument8 pagesCare of Clients with Problems in OxygenationRed StohlNo ratings yet
- Final NCP (Jannel)Document6 pagesFinal NCP (Jannel)Zed P. EstalillaNo ratings yet
- Acutronic Fabian HfoDocument21 pagesAcutronic Fabian Hfosermed50% (2)
- Toyota Forklift FBM 16-20-25 30 Repair ManualDocument22 pagesToyota Forklift FBM 16-20-25 30 Repair Manualdrroybarreramd141203wcr100% (109)
- Homeostasis of Blood Gas Levels ExplainedDocument5 pagesHomeostasis of Blood Gas Levels ExplainedFrancis YoonNo ratings yet
- Clinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test BankDocument36 pagesClinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test Bankgeincupola.06zi100% (22)
- Principles of Human Physiology 6th Edition Ebook PDFDocument61 pagesPrinciples of Human Physiology 6th Edition Ebook PDFbilly.sparks463100% (37)
- 8 L 5 1 RRR Practice QuestionsDocument8 pages8 L 5 1 RRR Practice QuestionsEliana FeingoldNo ratings yet
- Pulmonary Consolidation SyndromesDocument141 pagesPulmonary Consolidation SyndromesGiorgos Doukas KaranasiosNo ratings yet
- 1-First Aid Training Khmer & English (Basic)Document40 pages1-First Aid Training Khmer & English (Basic)Sor SethNo ratings yet