You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Haemodynamic Pocket GuideDocument2 pagesHaemodynamic Pocket GuideDarryl Betts85% (13)
- Cardiovascular System PhysiologyDocument109 pagesCardiovascular System PhysiologyKing kakaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Assessment of The Critically Ill PatientDocument5 pagesAssessment of The Critically Ill PatientCris John RicoNo ratings yet
- Traumatic Brain Injury UpdateDocument23 pagesTraumatic Brain Injury Updatejose luis iribarren100% (1)
- Hemodynamic Monitoring: Presented By, Alma SusanDocument19 pagesHemodynamic Monitoring: Presented By, Alma SusanAlma SusanNo ratings yet
- Principles of Doppler UltrasoundDocument47 pagesPrinciples of Doppler UltrasoundRolando Diaz100% (1)
- PulsioFlex PiCCO Data InterpretationDocument8 pagesPulsioFlex PiCCO Data InterpretationghuoiNo ratings yet
- Sslvd1-Eos2 - Mission BrochureDocument6 pagesSslvd1-Eos2 - Mission BrochureprasannasimhaNo ratings yet
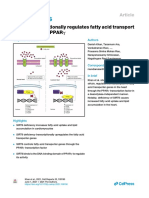
- SIRT6 PPAR Experssion PIIS2211124721005362Document20 pagesSIRT6 PPAR Experssion PIIS2211124721005362prasannasimhaNo ratings yet
- Mucosal Immunity in Viral DX Ann Immunol 2016Document37 pagesMucosal Immunity in Viral DX Ann Immunol 2016prasannasimhaNo ratings yet
- 2lewsi Dexter ASD 09.fullDocument17 pages2lewsi Dexter ASD 09.fullprasannasimhaNo ratings yet
- Mask H2O2 Sterilization IPIntJMedMicrobiolTropDis-7-4-232-236Document5 pagesMask H2O2 Sterilization IPIntJMedMicrobiolTropDis-7-4-232-236prasannasimhaNo ratings yet
- Linear AbridgedDocument145 pagesLinear AbridgedFrancisco BenítezNo ratings yet
- 02-07-2021 HMB EnglishDocument36 pages02-07-2021 HMB EnglishKiran SNNo ratings yet
- Mucosal Immunity in Viral DX Ann Immunol 2016Document37 pagesMucosal Immunity in Viral DX Ann Immunol 2016prasannasimhaNo ratings yet
- Basics of CPB: Praanna Simha Mohan RaoDocument35 pagesBasics of CPB: Praanna Simha Mohan Raoprasannasimha0% (1)
- Recent Trials Score 2019Document21 pagesRecent Trials Score 2019prasannasimhaNo ratings yet
- Mucosal Immunity in Viral DX Ann Immunol 2016Document37 pagesMucosal Immunity in Viral DX Ann Immunol 2016prasannasimhaNo ratings yet
- Iist Bond Format Undergraduate 2015Document5 pagesIist Bond Format Undergraduate 2015prasannasimhaNo ratings yet
- Cut Here Cut Here: Assembly InstructionsDocument1 pageCut Here Cut Here: Assembly InstructionsprasannasimhaNo ratings yet
- IIST Bond SpecimenDocument4 pagesIIST Bond SpecimenprasannasimhaNo ratings yet
- Flap Valved VSD Closure PrasannaDocument6 pagesFlap Valved VSD Closure PrasannaprasannasimhaNo ratings yet
- Improving Neuroprotection During Dhca, by Vicki Mahan, MD, Instructor in Surgery (PPT Slide Show)Document79 pagesImproving Neuroprotection During Dhca, by Vicki Mahan, MD, Instructor in Surgery (PPT Slide Show)prasannasimhaNo ratings yet
- Handbook Chapter 7Document4 pagesHandbook Chapter 7prasannasimhaNo ratings yet
- Answers To Questions: Activity 1: Hematocrit Determination (Pp. Pex-71-72)Document14 pagesAnswers To Questions: Activity 1: Hematocrit Determination (Pp. Pex-71-72)march33350% (2)
- Laporan Praktikum Faal Aplikasi PDFDocument13 pagesLaporan Praktikum Faal Aplikasi PDFSilvi ApreliaNo ratings yet
- Mechanisms of Blood Flow Restriction: The New Testament: YmposiumDocument8 pagesMechanisms of Blood Flow Restriction: The New Testament: YmposiumRosaneLacerdaNo ratings yet
- When Should Blood Pressure Be Measured?: Stage Approximate Age Systolic DiastolicDocument6 pagesWhen Should Blood Pressure Be Measured?: Stage Approximate Age Systolic DiastolicJesrel DelotaNo ratings yet
- 11 - Management Post Operative Low Cardiac Output SyndromeDocument46 pages11 - Management Post Operative Low Cardiac Output SyndromeNat SNo ratings yet
- The Clinical Significance of Whole Blood Viscosity in Cardiovascular MedicineDocument5 pagesThe Clinical Significance of Whole Blood Viscosity in Cardiovascular MedicineSolo NunooNo ratings yet
- Romer & Polkey 2008Document11 pagesRomer & Polkey 2008Ισαάκ ΑλέξανδροςNo ratings yet
- 1 Compression Therapy..Document43 pages1 Compression Therapy..Nermeen7No ratings yet
- Diafragma en ICCDocument13 pagesDiafragma en ICCMonserrat CruzNo ratings yet
- Preeklamsi 9Document22 pagesPreeklamsi 9Melda Amalia SikumbangNo ratings yet
- Intra-Arterial Catheterization For Invasive Monitoring: Indications, Insertion Techniques, and Interpretation - UpToDateDocument40 pagesIntra-Arterial Catheterization For Invasive Monitoring: Indications, Insertion Techniques, and Interpretation - UpToDatejuanpbagurNo ratings yet
- Kim1985 PDFDocument7 pagesKim1985 PDFfadwa lachkerNo ratings yet
- Law of Poiseuille: DescriptionDocument7 pagesLaw of Poiseuille: DescriptionRocio GCNo ratings yet
- Cardiovascular RegulationDocument40 pagesCardiovascular RegulationeliseudesafateNo ratings yet
- 2008 Tale of The Seven MaresDocument9 pages2008 Tale of The Seven MaresEduardo Alfredo Gutierrez PardoNo ratings yet
- Study Suggests Laughter Is Good For The HeartDocument5 pagesStudy Suggests Laughter Is Good For The Heartgloria500No ratings yet
- ZOOLOGYDocument7 pagesZOOLOGYAnand MishraNo ratings yet
- Pulsatile Oldroyd-B Blood Flow Dynamics in A Stenosed ArteryDocument9 pagesPulsatile Oldroyd-B Blood Flow Dynamics in A Stenosed ArteryJuana Valentina CamachoNo ratings yet
- Plasbumin 25 enDocument19 pagesPlasbumin 25 enlenaNo ratings yet
- TFG Víctor Fibla AntolíDocument47 pagesTFG Víctor Fibla AntolíVíctor Fibla AntolíNo ratings yet
- BLOOD and CIRCULATIONDocument11 pagesBLOOD and CIRCULATIONKert trocioNo ratings yet
- Cerebral HemodynamicsDocument63 pagesCerebral HemodynamicsMuhammad IhsanNo ratings yet
- Computer Methods and Programs in Biomedicine: Iqra Shahzadi, S. BilalDocument11 pagesComputer Methods and Programs in Biomedicine: Iqra Shahzadi, S. Bilalp ppNo ratings yet