You might also like
- Cinical Scenario CholelithiasisDocument2 pagesCinical Scenario CholelithiasisSarine GonzalezNo ratings yet
- Case ProtocolDocument4 pagesCase ProtocolEzekiel ArtetaNo ratings yet
- Danganan Protocol Ver 2Document7 pagesDanganan Protocol Ver 2FayeListancoNo ratings yet
- Post Op Case Studies: Malignant HyperthermiaDocument19 pagesPost Op Case Studies: Malignant HyperthermiaRenie SerranoNo ratings yet
- Case 1Document3 pagesCase 1Jeanny Lou Lago-FormosoNo ratings yet
- HELLP Syndrome Case Scenario 2AG1Document2 pagesHELLP Syndrome Case Scenario 2AG1JR Rolf NeuqeletNo ratings yet
- Diificult AirwayDocument13 pagesDiificult AirwayBhi-An BatobalonosNo ratings yet
- 12b Clinical Update Example 2018Document9 pages12b Clinical Update Example 2018Ana BienneNo ratings yet
- Case Protocol OB - H MOLEDocument3 pagesCase Protocol OB - H MOLEKim Adarem Joy ManimtimNo ratings yet
- Is 19Document7 pagesIs 19intan juitaNo ratings yet
- Spontaneous Splenic Rupture in A 21-Year Old Male Patient Patient: H.MDocument4 pagesSpontaneous Splenic Rupture in A 21-Year Old Male Patient Patient: H.MJoherNo ratings yet
- Medicina Legal: Ectopic Tubular Pregnancy in Post Tubectomy DeathDocument5 pagesMedicina Legal: Ectopic Tubular Pregnancy in Post Tubectomy DeathJorge Brouardel M ForenseNo ratings yet
- Course in The WardDocument5 pagesCourse in The WardAngelica Mercado SirotNo ratings yet
- Sample Name: Abscess With Cellulitis - Discharge SummaryDocument3 pagesSample Name: Abscess With Cellulitis - Discharge Summaryravip3366No ratings yet
- Surgical Case NCPDocument2 pagesSurgical Case NCPMaryjoy Gabriellee De La CruzNo ratings yet
- Splenic Trauma by DR Ali Resident SurgeonDocument56 pagesSplenic Trauma by DR Ali Resident SurgeonAli AbidNo ratings yet
- Jurnal Diverticulum MeckelDocument18 pagesJurnal Diverticulum MeckelAnissa Aulia AdjaniNo ratings yet
- Bar Dram 2000Document6 pagesBar Dram 2000Prasetyö AgungNo ratings yet
- Unit 5 Discussion SOAPDocument2 pagesUnit 5 Discussion SOAPMarcia100% (2)
- Client Nursing Care Plan for CholecystolithiasisDocument9 pagesClient Nursing Care Plan for CholecystolithiasisBelen SoleroNo ratings yet
- Inbound 988634411507331531Document7 pagesInbound 988634411507331531Jeannelle Landiza AmeninNo ratings yet
- CASE PRESENTATION Fracture of Distal HumerusDocument18 pagesCASE PRESENTATION Fracture of Distal HumerusIshika PaulNo ratings yet
- CasesDocument5 pagesCasesperiamaegan1No ratings yet
- Appendicitis SampleDocument15 pagesAppendicitis SampleChiqui Lao DumanhugNo ratings yet
- Left Side Appendix With Appendicitis 333Document3 pagesLeft Side Appendix With Appendicitis 333Medtext PublicationsNo ratings yet
- NCP GCP FinalDocument15 pagesNCP GCP FinalssilvozaNo ratings yet
- LL INDIA January 6th 2002 MD/MS Entrance Examination Questions With Suggested AnswersDocument26 pagesLL INDIA January 6th 2002 MD/MS Entrance Examination Questions With Suggested AnswersAnil KumarNo ratings yet
- Case PresentationDocument11 pagesCase PresentationHira Rafique100% (1)
- Laparoscopy AbscesoDocument7 pagesLaparoscopy AbscesoMedardo ApoloNo ratings yet
- Recto-Sigmoid Cancer Surgery Case ReportDocument11 pagesRecto-Sigmoid Cancer Surgery Case ReportHeshan SiriwardenaNo ratings yet
- Clinical Abstract (2nd Sem 1st Rotation)Document3 pagesClinical Abstract (2nd Sem 1st Rotation)Michael Gino SarenasNo ratings yet
- Example Discharge Letters PDFDocument5 pagesExample Discharge Letters PDFlanghal100% (1)
- Pathophysiology, Diagnosis,: and Treatment of The Postobstructive DiuresisDocument2 pagesPathophysiology, Diagnosis,: and Treatment of The Postobstructive DiuresisJohannes MarpaungNo ratings yet
- Usmle World QuestionsDocument6 pagesUsmle World Questionsdrktb100% (6)
- Substandard Neostigmindr Misal FinalDocument12 pagesSubstandard Neostigmindr Misal FinalusmisalNo ratings yet
- CASE SCENARIO AppendectomyDocument2 pagesCASE SCENARIO Appendectomybambam1aNo ratings yet
- CarbuncleDocument14 pagesCarbuncleMohd Anuar IbrahimNo ratings yet
- Ectopic Pregnancy in Uncommon SitesDocument10 pagesEctopic Pregnancy in Uncommon SitesrezachandraNo ratings yet
- Liver Abscess Risk FactorsDocument7 pagesLiver Abscess Risk FactorsJoan junioNo ratings yet
- Obstetrics Patient M.L. 26/F Date Admitted: December 17, 2018 Date Discharged: December 19, 2018 Informant: Patient Reliability: 80%Document6 pagesObstetrics Patient M.L. 26/F Date Admitted: December 17, 2018 Date Discharged: December 19, 2018 Informant: Patient Reliability: 80%Justin LamNo ratings yet
- A Case of Nonpharmacologic Conservative Management of Suspected Uncomplicated Subacute Appendicitis in An Adult MaleDocument5 pagesA Case of Nonpharmacologic Conservative Management of Suspected Uncomplicated Subacute Appendicitis in An Adult MaleTrueNorth Health Center75% (4)
- Pleural Effusion Case PresentationDocument78 pagesPleural Effusion Case PresentationAnie Zacarias100% (3)
- Spontaneous Vaginal Delivery Case StudyDocument2 pagesSpontaneous Vaginal Delivery Case StudychloeNo ratings yet
- Mortality and Morbidity Meeting PannirselvamDocument1 pageMortality and Morbidity Meeting PannirselvamMohammed SaleetNo ratings yet
- Portfolio Clinical ExemplarDocument6 pagesPortfolio Clinical Exemplarapi-365196865No ratings yet
- Managing Bilateral Ureterolithiasis: A Case StudyDocument3 pagesManaging Bilateral Ureterolithiasis: A Case StudyabinadivegaNo ratings yet
- JFP - 1986 09 - v23 - I3 - A Case of Chronic AppendicitisDocument2 pagesJFP - 1986 09 - v23 - I3 - A Case of Chronic AppendicitisBilalNo ratings yet
- Manila Doctors Hospital CCU Conference on Pulmonary EmbolismDocument5 pagesManila Doctors Hospital CCU Conference on Pulmonary EmbolismFayeListanco100% (1)
- Case Study July 19Document2 pagesCase Study July 19Vinay ShankerNo ratings yet
- Sample Questions For Emstrex 2012Document6 pagesSample Questions For Emstrex 2012Dr.2020100% (1)
- Pancreatitis ChronicDocument9 pagesPancreatitis ChronicGherca IzabellaNo ratings yet
- Wk15 NCP SrosaDocument3 pagesWk15 NCP SrosaSarah Ro SaNo ratings yet
- تقرير طبيDocument3 pagesتقرير طبيSmart Certified Translation ServicesNo ratings yet
- Gynaecological Case of Incomplete MiscarriageDocument10 pagesGynaecological Case of Incomplete Miscarriageemmanuel oduNo ratings yet
- Sujok InpancreatitisDocument70 pagesSujok InpancreatitisFedericoz Zarra100% (1)
- Peritonitis Generalisata Post Laparoskopi AppendiktomiDocument15 pagesPeritonitis Generalisata Post Laparoskopi AppendiktomiguterizalNo ratings yet
- Sample Dictation - SVDDocument1 pageSample Dictation - SVDmhariskurniawanNo ratings yet
- Different in the therapy of pressure negtotheeva single-useFrom EverandDifferent in the therapy of pressure negtotheeva single-useNo ratings yet
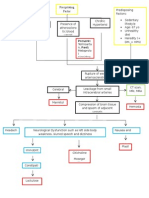
- Precipitating Factor: PresentDocument1 pagePrecipitating Factor: PresentShiela GuiquingNo ratings yet
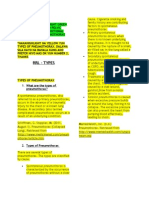
- Types (WC) of Pneumothorax and FracturesDocument6 pagesTypes (WC) of Pneumothorax and FracturesShiela GuiquingNo ratings yet
- Name Addres S Landlin e Mobile EmailDocument4 pagesName Addres S Landlin e Mobile EmailShiela GuiquingNo ratings yet
- Drink Water On Empty StomachDocument3 pagesDrink Water On Empty Stomachapi-25980492No ratings yet
- Premature InfantDocument91 pagesPremature InfantMCMNo ratings yet
- DRUG CALCULATIONS: KEY CONSIDERATIONSDocument42 pagesDRUG CALCULATIONS: KEY CONSIDERATIONSLovelyJoy Manalo100% (1)
- 671Document16 pages671ravensuichiroNo ratings yet
- Intro To Wastewater Collection and PumpingDocument84 pagesIntro To Wastewater Collection and PumpingMoh'd KhadNo ratings yet
- Effects of Vitamin B-12 Supplementation On Neurologic and Cognitive Function in Older People: A Randomized Controlled TrialDocument9 pagesEffects of Vitamin B-12 Supplementation On Neurologic and Cognitive Function in Older People: A Randomized Controlled TrialzuzuoonNo ratings yet
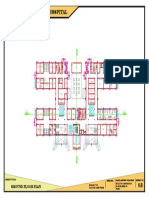
- 100-Bed General Hospital LayoutDocument1 page100-Bed General Hospital LayoutAshish chauhanNo ratings yet
- Needs - Human Needs Are The Basic Demands and Include Food, ClothingDocument3 pagesNeeds - Human Needs Are The Basic Demands and Include Food, ClothingChandi BalasooriyaNo ratings yet
- HISTORY AND PHYSICAL EXAMINATION (Putul)Document2 pagesHISTORY AND PHYSICAL EXAMINATION (Putul)Reshma Francis100% (1)
- Module 7 Health Insurance Types and ImportanceDocument10 pagesModule 7 Health Insurance Types and ImportanceKAH' CHISMISSNo ratings yet
- Being A Medical DoctorDocument14 pagesBeing A Medical DoctorMichael Bill GihonNo ratings yet
- Birads PosterDocument1 pageBirads PosterGopalarathnam BalachandranNo ratings yet
- Mindvalley - Superbrain Quest - SummaryDocument17 pagesMindvalley - Superbrain Quest - SummaryMagdy El ID100% (3)
- Spiced Oven-Baked Sweet Potato Fries With Salted Egg Yolk SauceDocument1 pageSpiced Oven-Baked Sweet Potato Fries With Salted Egg Yolk SaucetryabcdefNo ratings yet
- K55 MSDSDocument7 pagesK55 MSDSalocNo ratings yet
- Zhou 2008Document10 pagesZhou 2008zael18No ratings yet
- Introduction To Public Health... 1stDocument37 pagesIntroduction To Public Health... 1stNELSONJD20195100% (3)
- Newborn Care Volume 1 2020-1Document192 pagesNewborn Care Volume 1 2020-1Shyvonne PeirisNo ratings yet
- Emotional Dysregulation in Adult ADHD What Is The Empirical EvidenceDocument12 pagesEmotional Dysregulation in Adult ADHD What Is The Empirical EvidenceVo PeaceNo ratings yet
- Liquefied Gas Tanker Familiarisation Course: Operational & Support LevelDocument60 pagesLiquefied Gas Tanker Familiarisation Course: Operational & Support LevelAlpha OmegaNo ratings yet
- Common Assessment Framework FormDocument9 pagesCommon Assessment Framework FormparaypanNo ratings yet
- Adult Health - Soap Note 5Document3 pagesAdult Health - Soap Note 5api-546259691100% (3)
- IFUk en 310250 07 PDFDocument14 pagesIFUk en 310250 07 PDFKhaled AlkhawaldehNo ratings yet
- Vol3issue12018 PDFDocument58 pagesVol3issue12018 PDFpyrockerNo ratings yet
- NUST Hostel Admission Form New PDFDocument2 pagesNUST Hostel Admission Form New PDFMuhammad Waqas0% (1)
- Prepared By: Ulfat Amin MSC Pediatric NursingDocument25 pagesPrepared By: Ulfat Amin MSC Pediatric NursingAngelic khanNo ratings yet
- How To Make An ELearning ModuleDocument22 pagesHow To Make An ELearning ModulePradeep RawatNo ratings yet
- Technology and Livelihood Education: Quarter 1 - Module 4: CaregivingDocument20 pagesTechnology and Livelihood Education: Quarter 1 - Module 4: CaregivingIrine Irine100% (1)
- Heart Failure Lily ModifiedDocument57 pagesHeart Failure Lily ModifiedSabila FatimahNo ratings yet
- Table : Number of Population, Hospitals and Beds in All Over JordanDocument8 pagesTable : Number of Population, Hospitals and Beds in All Over JordanjNo ratings yet
- Bmjopen 2017 016402Document6 pagesBmjopen 2017 016402Ćatke TkećaNo ratings yet
- DSM 5Document35 pagesDSM 5Hemant KumarNo ratings yet
- Hazard Identification Risk Assessment Risk ControlDocument3 pagesHazard Identification Risk Assessment Risk Controle cubeNo ratings yet
- The Costly Business of DiscriminationDocument46 pagesThe Costly Business of DiscriminationCenter for American Progress100% (1)