You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The List InditexDocument126 pagesThe List InditexRezoanul Haque100% (2)
- COLLOIDAL GOLD RECIPE - CitrateDocument9 pagesCOLLOIDAL GOLD RECIPE - CitrateDevon Narok100% (4)
- ARI 700 StandardDocument19 pagesARI 700 StandardMarcos Antonio MoraesNo ratings yet
- Civil Society and Communities Declaration To End HIV: Human Rights Must Come FirstDocument7 pagesCivil Society and Communities Declaration To End HIV: Human Rights Must Come FirsthousingworksNo ratings yet
- Topic: Going To and Coming From Place of WorkDocument2 pagesTopic: Going To and Coming From Place of WorkSherry Jane GaspayNo ratings yet
- NYC LGBT Solidarity Rally Flyer For 2 4 17 ExternalDocument1 pageNYC LGBT Solidarity Rally Flyer For 2 4 17 ExternalhousingworksNo ratings yet
- Hillary Clinton Agenda and Meeting Notes 5.12.16Document9 pagesHillary Clinton Agenda and Meeting Notes 5.12.16Housing WorksNo ratings yet
- Housing Works "What's Your Voting Plan?!" Sheet 2018Document1 pageHousing Works "What's Your Voting Plan?!" Sheet 2018housingworksNo ratings yet
- May 2016 AIDS Advocates Consensus Policy Paper W EndorsersDocument17 pagesMay 2016 AIDS Advocates Consensus Policy Paper W EndorsershousingworksNo ratings yet
- #ICantBreathe/ Dec. 2014-Jan. 2015 Calls-to-Action Flyer, Housing Works Advocacy ActionsDocument2 pages#ICantBreathe/ Dec. 2014-Jan. 2015 Calls-to-Action Flyer, Housing Works Advocacy ActionshousingworksNo ratings yet
- Media Advisory 10.27 AIDS Community Press Conf RE Cuomo Ebola Quarantine FINALDocument1 pageMedia Advisory 10.27 AIDS Community Press Conf RE Cuomo Ebola Quarantine FINALhousingworksNo ratings yet
- Housing Works World AIDS Day 2014 CoalitionEvent FlyerSaveTheDate, EnglishDocument1 pageHousing Works World AIDS Day 2014 CoalitionEvent FlyerSaveTheDate, EnglishhousingworksNo ratings yet
- Braking AIDS Ride 2014. 9/12-9/14, Cheering Stations GuideDocument1 pageBraking AIDS Ride 2014. 9/12-9/14, Cheering Stations GuidehousingworksNo ratings yet
- Task Force End of AIDS NYS, Opening Remarks, 10.14.14, CKingDocument3 pagesTask Force End of AIDS NYS, Opening Remarks, 10.14.14, CKinghousingworksNo ratings yet
- Brooks - Brooklyn ONAP Presentation 8.8.14Document4 pagesBrooks - Brooklyn ONAP Presentation 8.8.14housingworksNo ratings yet
- LGBT Equality & Justice Day 2014 Event Info Flyer, April 29, 2014, AlbanyDocument1 pageLGBT Equality & Justice Day 2014 Event Info Flyer, April 29, 2014, AlbanyhousingworksNo ratings yet
- Advancing The National HIV/AIDS Strategy: Regional Listening SessionDocument4 pagesAdvancing The National HIV/AIDS Strategy: Regional Listening SessionhousingworksNo ratings yet
- NYC Festival of Forum and Legislative Theatre Cantgetright2014 PosterDocument1 pageNYC Festival of Forum and Legislative Theatre Cantgetright2014 PosterhousingworksNo ratings yet
- EV-H-A1R 54C - M - EN - 2014 - D - Heat Detector SalwicoDocument2 pagesEV-H-A1R 54C - M - EN - 2014 - D - Heat Detector SalwicoCarolinaNo ratings yet
- C 08 S 09Document8 pagesC 08 S 09Marnel Roy MayorNo ratings yet
- Aircraft Noise Management: Graduation Project Defense For The Diploma of Air Traffic Management EngineerDocument46 pagesAircraft Noise Management: Graduation Project Defense For The Diploma of Air Traffic Management Engineerchouchou chamaNo ratings yet
- SCI Fayette Greene..2007-2009 ViolationsDocument10 pagesSCI Fayette Greene..2007-2009 ViolationsHRCFedUpNo ratings yet
- Development of Elevator Ropes: Tech Tip 15Document2 pagesDevelopment of Elevator Ropes: Tech Tip 15أحمد دعبسNo ratings yet
- Blessing of The Advent WreathDocument3 pagesBlessing of The Advent WreathLloyd Paul ElauriaNo ratings yet
- Application of Knowledge QuestionsDocument16 pagesApplication of Knowledge QuestionsElllie TattersNo ratings yet
- Gastroschisis and Omphalocele PDFDocument8 pagesGastroschisis and Omphalocele PDFUtama puteraNo ratings yet
- A0002 HR Operations Manual Quick Reference FileDocument6 pagesA0002 HR Operations Manual Quick Reference FileRaffy Pax Galang RafaelNo ratings yet
- Evolution of Fluidized Bed TechnologyDocument17 pagesEvolution of Fluidized Bed Technologyika yuliyani murtiharjonoNo ratings yet
- Selectivities in Ionic Reductions of Alcohols and Ketones With Triethyisilane - Trifluoroacetic AcidDocument4 pagesSelectivities in Ionic Reductions of Alcohols and Ketones With Triethyisilane - Trifluoroacetic AcidJan Andre EriksenNo ratings yet
- EML Prosedur ManualDocument1,019 pagesEML Prosedur Manualzrohim bapetenkfk2023No ratings yet
- Molecular MechanicsDocument26 pagesMolecular MechanicsKarthi ShanmugamNo ratings yet
- Unit Plan Adult Health Nursing Unit IIDocument7 pagesUnit Plan Adult Health Nursing Unit IIDelphy VargheseNo ratings yet
- Theory of Accounts On Business CombinationDocument2 pagesTheory of Accounts On Business CombinationheyNo ratings yet
- Articulo de Las 3 Tesis Por BrowDocument30 pagesArticulo de Las 3 Tesis Por BrowJHIMI DEIVIS QUISPE ROQUENo ratings yet
- Boge FLEX PET SystemsDocument4 pagesBoge FLEX PET SystemsAir Repair, LLCNo ratings yet
- GLYSANTIN+G48+bg+IN 000000000030667689 SDS GEN US en 8-1Document11 pagesGLYSANTIN+G48+bg+IN 000000000030667689 SDS GEN US en 8-1Ali RidloNo ratings yet
- LR-360KAS-BROCHURE-LNG Sampling SystemsDocument4 pagesLR-360KAS-BROCHURE-LNG Sampling SystemsIdehen KelvinNo ratings yet
- The Man Booker PrizeDocument2 pagesThe Man Booker PrizeChu Hòa Bình100% (1)
- CW Catalogue Cables and Wires A4 En-2Document1,156 pagesCW Catalogue Cables and Wires A4 En-2Ovidiu PuieNo ratings yet
- Jis C 8156-2017, EngDocument32 pagesJis C 8156-2017, Eng7620383tlNo ratings yet
- AST CatalogDocument44 pagesAST CatalogCRISTIANNo ratings yet
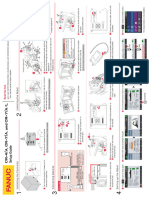
- CR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)Document1 pageCR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)lidiia.pavlkukNo ratings yet
- RA ELECTRONICSTECH CEBU Apr2019 PDFDocument12 pagesRA ELECTRONICSTECH CEBU Apr2019 PDFPhilBoardResultsNo ratings yet
- AIPMT 2009 ExamDocument25 pagesAIPMT 2009 ExamMahesh ChavanNo ratings yet