You might also like
- Humanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperFrom EverandHumanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperNo ratings yet
- Care of The DyingDocument4 pagesCare of The Dyingprokuno89% (9)
- Hospice and PallativeDocument38 pagesHospice and PallativeVhe Pacatang100% (1)
- Family Medicine - Hospice Care and PalliationDocument1 pageFamily Medicine - Hospice Care and Palliationk.n.e.d.No ratings yet
- Introduction To Palliative Care NursingDocument3 pagesIntroduction To Palliative Care NursingAbigail LonoganNo ratings yet
- Journal of Surgical NurseDocument8 pagesJournal of Surgical NurseWahyu WeraNo ratings yet
- Konsep Palliative Care Pada AnakDocument48 pagesKonsep Palliative Care Pada AnakDayu Dani100% (1)
- Hospice & Palliative CareDocument21 pagesHospice & Palliative CareAmy100% (1)
- Hospice Care (End of Life Care) For Terminal Illness - Case Study SampleDocument19 pagesHospice Care (End of Life Care) For Terminal Illness - Case Study Samplepeng kulongNo ratings yet
- Hospice Palliative CareDocument22 pagesHospice Palliative CareKim GonzalesNo ratings yet
- El1 - Palliative & Hospice Care in The PhilippinesDocument49 pagesEl1 - Palliative & Hospice Care in The PhilippinesStudentnurseMj50% (4)
- Nursing Care at The End of Life PDFDocument139 pagesNursing Care at The End of Life PDFPradeep JNANo ratings yet
- Advancing Palliative End of Life Care in Alberta ReportDocument23 pagesAdvancing Palliative End of Life Care in Alberta ReportCTV News EdmontonNo ratings yet
- End of Life CareDocument11 pagesEnd of Life CareBelindaNo ratings yet
- Pain Management in Palliative CareDocument22 pagesPain Management in Palliative Carepuchio100% (1)
- End of Life CareDocument25 pagesEnd of Life CareMeenu DograNo ratings yet
- End of Life - Hospice CareDocument9 pagesEnd of Life - Hospice CareKaloy KamaoNo ratings yet
- Hospice Care in The Nursing HomeDocument73 pagesHospice Care in The Nursing Homeraul nino Moran100% (1)
- Palliative NursingDocument31 pagesPalliative NursingNyein MohNo ratings yet
- Hospice Care PlanDocument9 pagesHospice Care PlanAmanda SimpsonNo ratings yet
- Hospice CareDocument2 pagesHospice CareSamuel YoungNo ratings yet
- NCM 114 Mod2Document6 pagesNCM 114 Mod2Samantha BolanteNo ratings yet
- End of Life CareDocument80 pagesEnd of Life CareRakesh MohanNo ratings yet
- End of Life Care FDocument84 pagesEnd of Life Care FJhunnie NuquiNo ratings yet
- Clinical Practice Guidelines For Quality Palliative Care (National Consensus Project)Document76 pagesClinical Practice Guidelines For Quality Palliative Care (National Consensus Project)NCP86% (7)
- 2.4 Hospice and Palliative CareDocument93 pages2.4 Hospice and Palliative CareCzara DyNo ratings yet
- (DR Joyce Zerwekh) Nursing Care at The End of LifeDocument472 pages(DR Joyce Zerwekh) Nursing Care at The End of LifeSubbie Outlier83% (6)
- Quizzes in CHNDocument2 pagesQuizzes in CHNMichelle GambolNo ratings yet
- Palliative Care 11918Document69 pagesPalliative Care 11918meldelsNo ratings yet
- Community Health NursingDocument140 pagesCommunity Health NursingPrince Jhessie L. Abella67% (3)
- End-Of-Life Decision Making Across CulturesDocument15 pagesEnd-Of-Life Decision Making Across CulturesPamNo ratings yet
- Community Health NursingDocument516 pagesCommunity Health NursingFabby Vitacion Tan75% (4)
- Revised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)Document6 pagesRevised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)NATHANIEL YERINo ratings yet
- End of Life IssuesDocument8 pagesEnd of Life IssuesJo RanamoNo ratings yet
- NCM 101 Lecture Notes Prelims Handout 2: GreywolfredDocument9 pagesNCM 101 Lecture Notes Prelims Handout 2: GreywolfredRI NANo ratings yet
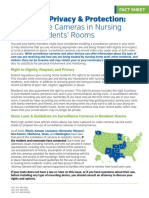
- Cameras in Nursing HomesDocument2 pagesCameras in Nursing HomesWews WebStaffNo ratings yet
- Community Health Nursing ProcessDocument35 pagesCommunity Health Nursing Processdave100% (1)
- Roles and Functions of The NurseDocument115 pagesRoles and Functions of The Nurse3amabelle arevalo0% (1)
- The Nurses Role in Palliative Care A QualitativeDocument18 pagesThe Nurses Role in Palliative Care A Qualitativesukarni84sgdNo ratings yet
- Charting GuideDocument2 pagesCharting GuideCherry Magadia100% (3)
- Mental Health Nursing HandoutDocument25 pagesMental Health Nursing HandoutJamaica Manuel IglesiasNo ratings yet
- Psychiatric Nursing Notes: Settings For Psychiatric CareDocument31 pagesPsychiatric Nursing Notes: Settings For Psychiatric Caresurviving nursing schoolNo ratings yet
- Palliative Care - End of Life Care - Northern HealthDocument8 pagesPalliative Care - End of Life Care - Northern HealthDiklatpimempat AngkatanlimabelasNo ratings yet
- Hospice Care Centre (": Shanti Avedna Sadan)Document14 pagesHospice Care Centre (": Shanti Avedna Sadan)Anam AnsariNo ratings yet
- B. The Absence of Disease.: C. EmergencyDocument7 pagesB. The Absence of Disease.: C. Emergencyエド パジャロンNo ratings yet
- Principles of Palliative and HospiceDocument15 pagesPrinciples of Palliative and HospiceChucky Vergara100% (1)
- End of Life ManualDocument238 pagesEnd of Life ManualJeffery TaylorNo ratings yet
- Cure Palliative 1Document64 pagesCure Palliative 1Mr. LNo ratings yet
- Fundamentals of NursingDocument27 pagesFundamentals of NursingRobeth OrbisoNo ratings yet
- To Study Modern Hospice Designs:The Architecture of Palliative Care and HealingDocument4 pagesTo Study Modern Hospice Designs:The Architecture of Palliative Care and HealingPRACHI MANTRI100% (1)
- Unit 9-Personal Care and GroomingDocument110 pagesUnit 9-Personal Care and Groomingtau88No ratings yet
- Palliative Care: Mrs. Grace Lydia Asst - Professor OacnDocument133 pagesPalliative Care: Mrs. Grace Lydia Asst - Professor OacnSophia Alexa Cassandra AlcantaraNo ratings yet
- Emergency NursingDocument5 pagesEmergency Nursingchelljynxie100% (2)
- CHNDocument38 pagesCHNLouie John AbilaNo ratings yet
- Community Case: Faith-Based CommunityDocument1 pageCommunity Case: Faith-Based CommunityFatima G ReyesNo ratings yet
- A Hospice Guide Book: Hospice Care: a Wise Choice Providing Quality Comfort Care Through the End of Life's JourneyFrom EverandA Hospice Guide Book: Hospice Care: a Wise Choice Providing Quality Comfort Care Through the End of Life's JourneyNo ratings yet
- Notes on Nursing - What It Is, and What It Is Not: With a Chapter From 'Beneath the Banner, Being Narratives of Noble Lives and Brave Deeds' by F. J. CrossFrom EverandNotes on Nursing - What It Is, and What It Is Not: With a Chapter From 'Beneath the Banner, Being Narratives of Noble Lives and Brave Deeds' by F. J. CrossNo ratings yet
- Housecalls 101: Policy and Procedure Manual for Medical Home VisitsFrom EverandHousecalls 101: Policy and Procedure Manual for Medical Home VisitsNo ratings yet
- Talking Therapy: Knowledge and Power in American Psychiatric NursingFrom EverandTalking Therapy: Knowledge and Power in American Psychiatric NursingNo ratings yet
- Skill Development: Semester - IvDocument53 pagesSkill Development: Semester - IvKARANNo ratings yet
- Processing of Persuasive In-Group MessagesDocument11 pagesProcessing of Persuasive In-Group MessagesJoyce TanNo ratings yet
- Analysis of Error in Math.Document9 pagesAnalysis of Error in Math.CYNTHIA QUEEN TAN MANGGOBNo ratings yet
- My ReflectionDocument6 pagesMy ReflectionJai Ejumpz JaidiNo ratings yet
- Chapter - II Review of Literature Review of LiteratureDocument24 pagesChapter - II Review of Literature Review of LiteratureeshuNo ratings yet
- ss10 Term 2 Assessment 2Document3 pagesss10 Term 2 Assessment 2api-288515796No ratings yet
- Contemporary Management 11th Edition Test Bank Chapter 14Document49 pagesContemporary Management 11th Edition Test Bank Chapter 14Manal Al OjailiNo ratings yet
- Peer Influence and Classroom Management Among Bse-Biology StudentsDocument52 pagesPeer Influence and Classroom Management Among Bse-Biology StudentsJenny Villa AlcantaraNo ratings yet
- Interference TheoryDocument3 pagesInterference TheoryMJ JOYCENo ratings yet
- 101-115 PPT QuestionsDocument42 pages101-115 PPT QuestionsGlennette Claire Almora100% (1)
- Cross (1998) Music Analysis and Music Perception PDFDocument19 pagesCross (1998) Music Analysis and Music Perception PDFMelisa CanteroNo ratings yet
- Interpersonal PerceptionDocument2 pagesInterpersonal PerceptionJhay0% (1)
- Policy and Guidelines On Protecting Children in School From Abuse, Violence, Exploitation, Discrimination, Bullying and Other Forms of AbuseDocument33 pagesPolicy and Guidelines On Protecting Children in School From Abuse, Violence, Exploitation, Discrimination, Bullying and Other Forms of AbuseMa'am Ja Nheez RG100% (1)
- Relational Dialectics Theory: MontgomeryDocument3 pagesRelational Dialectics Theory: MontgomeryRocelle AlcaparazNo ratings yet
- Teachers' Morale and Its Impact To Their Working EfficiencyDocument8 pagesTeachers' Morale and Its Impact To Their Working EfficiencyRad John BelarminoNo ratings yet
- Leisure Sciences: An Interdisciplinary JournalDocument14 pagesLeisure Sciences: An Interdisciplinary JournalTroy CabrillasNo ratings yet
- Human Resource ManagementDocument22 pagesHuman Resource ManagementRohit ChaudharyNo ratings yet
- Session 1: Early Language Literacy and Numeracy: Pre-TestDocument40 pagesSession 1: Early Language Literacy and Numeracy: Pre-TestGly Pascual Asuncion100% (1)
- Ignatius As NeetDocument14 pagesIgnatius As Neetapi-454747503No ratings yet
- Pastoral Psychology: Pastors Clergy CongregationsDocument21 pagesPastoral Psychology: Pastors Clergy CongregationsChe'gu JamalNo ratings yet
- Relevance PyschologyDocument2 pagesRelevance Pyschologygeetkumar18No ratings yet
- Slide1:: Script With CuesDocument3 pagesSlide1:: Script With CuesendersiteNo ratings yet
- Family ProblemDocument9 pagesFamily Problemmicah reluaoNo ratings yet
- Muslim Religiosity-Personality Inventory Test ResultsDocument31 pagesMuslim Religiosity-Personality Inventory Test ResultsAhmad RizaNo ratings yet
- Tami Jo Redinger Cover LetterDocument1 pageTami Jo Redinger Cover Letterapi-296395535No ratings yet
- Module 3 Multiple Choice QuizDocument6 pagesModule 3 Multiple Choice QuizMag9191No ratings yet
- The Effects of Music Tempo On Memory Performance Using Maintenance Rehearsal and ImageryDocument19 pagesThe Effects of Music Tempo On Memory Performance Using Maintenance Rehearsal and ImagerySunway University100% (1)
- Cel 2106 SCL Worksheet Week 2Document3 pagesCel 2106 SCL Worksheet Week 2Anya NieveNo ratings yet
- Alcohol Addiction TreatmentDocument12 pagesAlcohol Addiction Treatmentkuna2750% (2)
- Bowling ActivityDocument3 pagesBowling Activityapi-360253809No ratings yet