You might also like
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- The Effect of Probiotics in Prevention of Necrotising Enterocolitis in Preterm Neonates in Comparison With Control GroupDocument4 pagesThe Effect of Probiotics in Prevention of Necrotising Enterocolitis in Preterm Neonates in Comparison With Control GroupchachaNo ratings yet
- Acute PancreatitisDocument9 pagesAcute PancreatitisJayari Cendana PutraNo ratings yet
- Van Puffelen 2018 Oi 180133Document11 pagesVan Puffelen 2018 Oi 180133Bunga Nur AnnisaNo ratings yet
- Enteral Nutrition in The Critically Ill Marik PDFDocument8 pagesEnteral Nutrition in The Critically Ill Marik PDFCami Cuevas VergaraNo ratings yet
- Allergy and Constipation Borelli Am J Gastroenterol 2009 PDFDocument10 pagesAllergy and Constipation Borelli Am J Gastroenterol 2009 PDFVanessadeOliveiraNo ratings yet
- Digest: Predictors of Failure of Pneumatic Dilatation in AchalasiaDocument3 pagesDigest: Predictors of Failure of Pneumatic Dilatation in AchalasiaDian Eka PermataNo ratings yet
- Cisapride Use in Pediatric Patients With Intestinal Failure and Its Impact On Progression of Enteral NutritionDocument6 pagesCisapride Use in Pediatric Patients With Intestinal Failure and Its Impact On Progression of Enteral Nutritionmango91286No ratings yet
- Clinical Nutrition: Randomized Control TrialsDocument5 pagesClinical Nutrition: Randomized Control TrialsBby AdelinaNo ratings yet
- Bolus Vs Continuous Nasogastric Feeds in Mechanically VentilatedDocument17 pagesBolus Vs Continuous Nasogastric Feeds in Mechanically VentilatedMirzania Mahya FathiaNo ratings yet
- Mathur 2015Document7 pagesMathur 2015Maximiliano OliveraNo ratings yet
- Nqy 012Document6 pagesNqy 012Pablo MoraNo ratings yet
- Inicio de La Alimentacion Parenteral en El Niño Criticamente EnfermoDocument10 pagesInicio de La Alimentacion Parenteral en El Niño Criticamente EnfermoNATALIA LEMOS CALLENo ratings yet
- A. Brief Resume of Intended WorkDocument6 pagesA. Brief Resume of Intended WorkRabi DhakalNo ratings yet
- Reading Journal ALYADocument14 pagesReading Journal ALYAAlya AnnisaNo ratings yet
- Comparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialDocument5 pagesComparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialVindee VictoryNo ratings yet
- ProbiotikDocument9 pagesProbiotikmasitah nasutionNo ratings yet
- Estacion EsDocument12 pagesEstacion EsLuis Quito CaroNo ratings yet
- Alimentary TractDocument8 pagesAlimentary Tractgrace liwantoNo ratings yet
- Jurnal Probiotik 1Document5 pagesJurnal Probiotik 1Yose Rinaldy NababanNo ratings yet
- Jurnal 3 Fater 2Document8 pagesJurnal 3 Fater 2ANDIANY CAHYANTY TAHIRNo ratings yet
- Bifidobacterium and Enteral Feeding in Preterm Infants: Cluster-Randomized TrialDocument6 pagesBifidobacterium and Enteral Feeding in Preterm Infants: Cluster-Randomized TrialnashwaNo ratings yet
- 2010 Early CPAP Vs Surfactant in EPTI NEJMDocument10 pages2010 Early CPAP Vs Surfactant in EPTI NEJMFiorella VilcaNo ratings yet
- Can Tey 2015Document4 pagesCan Tey 2015irenesmbNo ratings yet
- ContentServer - Asp 110Document7 pagesContentServer - Asp 110kookiescreamNo ratings yet
- Role of Dexamethasone in Neonatal Meningitis 2012Document6 pagesRole of Dexamethasone in Neonatal Meningitis 2012jose alberto gamboaNo ratings yet
- Early Feeding in Acute Pancreatitis in Children A Randomized Controlled TrialDocument9 pagesEarly Feeding in Acute Pancreatitis in Children A Randomized Controlled TrialvalenciaNo ratings yet
- Faecal calprotectin (FC) in babies born to oher with or without IBDocument2 pagesFaecal calprotectin (FC) in babies born to oher with or without IBMartinaNo ratings yet
- Early aggressive feeding in VLBW neonatesDocument5 pagesEarly aggressive feeding in VLBW neonatesCandy RevolloNo ratings yet
- Probioticos - Enterocolitis Necrozante en PrematurosDocument7 pagesProbioticos - Enterocolitis Necrozante en PrematurosJuan David Montua ValenciaNo ratings yet
- Total Parenteral Nutrition: Potion or Poison?: Special ArticleDocument4 pagesTotal Parenteral Nutrition: Potion or Poison?: Special ArticleJavier VegaNo ratings yet
- Direct Hyperbilirubinemia in Newborns With GastroschisisDocument9 pagesDirect Hyperbilirubinemia in Newborns With GastroschisisAnisaa GayatriNo ratings yet
- Contoh UTBK SoshumDocument6 pagesContoh UTBK SoshumsalshabilaNo ratings yet
- Recurrent NEC-like enterocolitis in preterms linked to milk proteinDocument3 pagesRecurrent NEC-like enterocolitis in preterms linked to milk proteinJuwita PratiwiNo ratings yet
- Probiotics and Preterm Infants A Position Paper.26 ShareDocument17 pagesProbiotics and Preterm Infants A Position Paper.26 Shareendy tovarNo ratings yet
- Development and Current Use of Parenteral Nutrition in Critical Care - An Opinion PaperDocument10 pagesDevelopment and Current Use of Parenteral Nutrition in Critical Care - An Opinion PaperDwi Ditia ZazzoraNo ratings yet
- E794 FullDocument10 pagesE794 FullMaria Camila Ramírez GutiérrezNo ratings yet
- Divya Thesis Final (30th Jan)Document26 pagesDivya Thesis Final (30th Jan)smalaparaNo ratings yet
- Early Total Enteral Feeding in Stable Very Low Birth Weight Infants: A Before and After StudyDocument7 pagesEarly Total Enteral Feeding in Stable Very Low Birth Weight Infants: A Before and After StudySupriya M A SuppiNo ratings yet
- 1 Predict NeoDocument5 pages1 Predict NeoGary Carhuamaca LopezNo ratings yet
- Hilditch 2018Document3 pagesHilditch 2018rezkyfikriNo ratings yet
- Acta PaediatricaDocument13 pagesActa PaediatricaDefranky TheodorusNo ratings yet
- Sii ArtículoDocument5 pagesSii ArtículoMonserrat Garduño FonsecaNo ratings yet
- Art:10.1007/s00431 007 0419 XDocument8 pagesArt:10.1007/s00431 007 0419 XDini NanamiNo ratings yet
- An Evaluation of Chest Physiotherapy in The Management of Acute Bronchiolitis Changing Clinical Practice PDFDocument6 pagesAn Evaluation of Chest Physiotherapy in The Management of Acute Bronchiolitis Changing Clinical Practice PDFbuku fisioNo ratings yet
- NAC Effect on Inflammation in Pediatric Kidney InfectionDocument9 pagesNAC Effect on Inflammation in Pediatric Kidney Infectionstrawberry cheesecakeNo ratings yet
- Nejmoa1911998 PDFDocument11 pagesNejmoa1911998 PDFStella NoviaNo ratings yet
- AAActa Paediatr 2019 Jan 108 (1) 12Document8 pagesAAActa Paediatr 2019 Jan 108 (1) 12Clau CLópezNo ratings yet
- Objective Study Design: M P, MD, S B. K, MD, K L. A, P D, H S. B, MDDocument6 pagesObjective Study Design: M P, MD, S B. K, MD, K L. A, P D, H S. B, MDSY LodhiNo ratings yet
- Probiotik Clinical Applications in Gastrointestinal DiseaseDocument29 pagesProbiotik Clinical Applications in Gastrointestinal DiseaseDwi Feri HariyantoNo ratings yet
- Alimentación Enteral Luego de Exposición A Sedantes y Analgésicos en Muy Bajo PesoDocument6 pagesAlimentación Enteral Luego de Exposición A Sedantes y Analgésicos en Muy Bajo PesoAlfredo PérezNo ratings yet
- tugasDocument12 pagestugasLola SantiaNo ratings yet
- Early Enteral Feeding and Nosocomial Sepsis in Very Low Birthweight InfantsDocument4 pagesEarly Enteral Feeding and Nosocomial Sepsis in Very Low Birthweight InfantsaripbudiboyNo ratings yet
- Protein Moringa OleiferaDocument20 pagesProtein Moringa OleiferaAnxiety DisorderNo ratings yet
- Penting Banget DibacaDocument15 pagesPenting Banget DibacaDominikus Raditya AtmakaNo ratings yet
- Prophylactic Use of Fluconazole in Very Premature InfantsDocument7 pagesProphylactic Use of Fluconazole in Very Premature InfantsYurika Elizabeth SusantiNo ratings yet
- Ref 1Document7 pagesRef 1Tiago BaraNo ratings yet
- Effect of Bacterial Lysate and The Immunologic Mechanism in Treating BronchiolitisDocument5 pagesEffect of Bacterial Lysate and The Immunologic Mechanism in Treating BronchiolitisAbi CardenasNo ratings yet
- Changes in Fecal Microbiota and Metabolomics in A Child With JIA Responding To Two Treatment Periods With Exclusive Enteral NutritionDocument6 pagesChanges in Fecal Microbiota and Metabolomics in A Child With JIA Responding To Two Treatment Periods With Exclusive Enteral Nutritiondoc0814No ratings yet
- Randomized Controlled Trial of Talactoferrin Oral Solution in Preterm InfantsDocument9 pagesRandomized Controlled Trial of Talactoferrin Oral Solution in Preterm InfantsSardono WidinugrohoNo ratings yet
- IPL 2012 ScheduleDocument2 pagesIPL 2012 SchedulepatelkinjeshNo ratings yet
- WPAD Final BrochureDocument2 pagesWPAD Final BrochureshalukiriNo ratings yet
- KasaiDocument7 pagesKasaishalukiriNo ratings yet
- Perineal SensationDocument17 pagesPerineal SensationshalukiriNo ratings yet
- Final - PESUCON-2010 - BrochureDocument3 pagesFinal - PESUCON-2010 - BrochureshalukiriNo ratings yet
- Congenital Anomaly of PancreasDocument38 pagesCongenital Anomaly of PancreasshalukiriNo ratings yet
- Immunisation Schedule IndianDocument4 pagesImmunisation Schedule Indiandrvinay83No ratings yet
- Tuberculosis: by Rohma XI A2, Roll No.-2Document15 pagesTuberculosis: by Rohma XI A2, Roll No.-2fur ballNo ratings yet
- Cellular AdaptationsDocument16 pagesCellular AdaptationsROHITHNo ratings yet
- PDQ HistoDocument225 pagesPDQ HistoHtike Myat PhyuNo ratings yet
- (MT 57) PARA - Pathogenic ProtozoaDocument5 pages(MT 57) PARA - Pathogenic ProtozoaLiana JeonNo ratings yet
- A Color Atlas of Poultry Diseases by J L VegadDocument144 pagesA Color Atlas of Poultry Diseases by J L VegadId DyNo ratings yet
- Evaluation of Dysuria in AdultsDocument8 pagesEvaluation of Dysuria in AdultspapermintNo ratings yet
- Theory Part B-20.7.2016Document58 pagesTheory Part B-20.7.2016KaniyaTabinaNo ratings yet
- FinalpracDocument26 pagesFinalpracmzunl25476No ratings yet
- Seminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsDocument14 pagesSeminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsAlexander ArguelloNo ratings yet
- Blood and ImmunityDocument4 pagesBlood and ImmunityBok Delos Santos0% (1)
- Locomotion and Movement: SolutionsDocument22 pagesLocomotion and Movement: SolutionsvarshavishuNo ratings yet
- Ebook - Understanding Immune Cell Function in Cancer - IsoPlexisDocument7 pagesEbook - Understanding Immune Cell Function in Cancer - IsoPlexisJ VelazcoNo ratings yet
- Shigella SonneiDocument2 pagesShigella SonneiGuillame SawadogoNo ratings yet
- Mushtaq Ahmad: Running Head: REFLECTIVE LOG 1Document5 pagesMushtaq Ahmad: Running Head: REFLECTIVE LOG 1Shafiq Ur RahmanNo ratings yet
- Genetic SL Test: (100 Marks)Document19 pagesGenetic SL Test: (100 Marks)Ritika GulguliaNo ratings yet
- Enumeration of Bacteria in Milk Samples and Presumptive Test For ColiformsDocument5 pagesEnumeration of Bacteria in Milk Samples and Presumptive Test For ColiformsAlda YanaNo ratings yet
- Protein Synthesis: How Do We Get Proteins From A Bunch of A's, T'S, C's and G's in DNA??Document33 pagesProtein Synthesis: How Do We Get Proteins From A Bunch of A's, T'S, C's and G's in DNA??jodyjodzNo ratings yet
- Student Exploration: MeiosisDocument8 pagesStudent Exploration: MeiosisAshtyn CurnowNo ratings yet
- Cells: The Living Units: Chapter 3 - Part DDocument10 pagesCells: The Living Units: Chapter 3 - Part DJonathan HigginbothamNo ratings yet
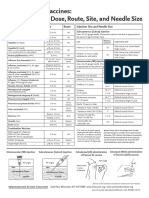
- Administering Vaccines: Dose, Route, Site and Needle Size GuideDocument1 pageAdministering Vaccines: Dose, Route, Site and Needle Size GuideKate Lucernas MayugaNo ratings yet
- Dictionary of Biomedical Research 4080 Words 155pDocument155 pagesDictionary of Biomedical Research 4080 Words 155pMSKCNo ratings yet
- DNA To Proteins (Insulin)Document4 pagesDNA To Proteins (Insulin)Gabby SalazarNo ratings yet
- Chapter19 Transplantation ImmunologyDocument77 pagesChapter19 Transplantation Immunologymalesh123No ratings yet
- 8.1 Organisation of Nervous System & Nerve CellsDocument71 pages8.1 Organisation of Nervous System & Nerve Cells5kj9ysmf24No ratings yet
- Food Microbiology NotesDocument11 pagesFood Microbiology NotesDrHassan AbdirahmanNo ratings yet
- Rhizopoda: Morphology and Characteristics of Common Intestinal ProtistsDocument24 pagesRhizopoda: Morphology and Characteristics of Common Intestinal ProtistsMuhammad Iqbal AnandNo ratings yet
- Mitochondrial DNA and Disease: A Concise ReviewDocument12 pagesMitochondrial DNA and Disease: A Concise Reviewpijush ghoshNo ratings yet
- Laporan Kasus Aiman KamilaDocument16 pagesLaporan Kasus Aiman KamilazzooooeeeeeeNo ratings yet
- AQA AS Biology Revision ChecklistDocument18 pagesAQA AS Biology Revision ChecklistMuhammadNo ratings yet
- Viral Blips During Suppressive Antiretroviral Treatment Are Associated With High Baseline HIV-1 RNA LevelsDocument9 pagesViral Blips During Suppressive Antiretroviral Treatment Are Associated With High Baseline HIV-1 RNA Levelssarah alatasNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (31)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)