You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Ashley Jones RN ResumeDocument1 pageAshley Jones RN Resumeapi-299649525100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Anamnesis & PemfisDocument81 pagesAnamnesis & PemfisFikriYTNo ratings yet
- At The DOCTOR Dialogues and Vocabulary ListDocument12 pagesAt The DOCTOR Dialogues and Vocabulary ListMax Tapia CastilloNo ratings yet
- Stress: Dr. Jayesh PatidarDocument56 pagesStress: Dr. Jayesh PatidarDr. Jayesh Patidar100% (2)
- Philippine Diabetes Prevention ProgramDocument19 pagesPhilippine Diabetes Prevention Programkoala100% (1)
- Enteral Feeding Nursing Care PlanDocument2 pagesEnteral Feeding Nursing Care PlanChebz Zy0% (1)
- Dialysis in Older PatientsDocument220 pagesDialysis in Older PatientsMiguel Angel Molinero100% (1)
- HSS Sotw 2017-18 ArDocument98 pagesHSS Sotw 2017-18 Arlf515No ratings yet
- Project Management HealthcareDocument29 pagesProject Management Healthcareiyad.alsabiNo ratings yet
- Communicating With Patients From Different Cultural BackgroundDocument24 pagesCommunicating With Patients From Different Cultural BackgroundRiska Aprilia100% (1)
- IDS Inmediate Dentin Sealing For Tooth Preparations... Magne 2014Document2 pagesIDS Inmediate Dentin Sealing For Tooth Preparations... Magne 2014Angie HernándezNo ratings yet
- AXR PresentationDocument30 pagesAXR PresentationLalit KumarNo ratings yet
- IVMS ICM-Heart MurmursDocument22 pagesIVMS ICM-Heart MurmursMarc Imhotep Cray, M.D.No ratings yet
- Nerve Entrapment - UpdateDocument17 pagesNerve Entrapment - UpdatealobrienNo ratings yet
- A Soft-Tissue Cephalometric Analysis and Its Use in Orthodontic Treatment Planning. Part IDocument28 pagesA Soft-Tissue Cephalometric Analysis and Its Use in Orthodontic Treatment Planning. Part IJorge Ramírez100% (1)
- Gastritis Treatment PlanDocument2 pagesGastritis Treatment PlanSuresh ThanneruNo ratings yet
- Practice Test On NutritionDocument6 pagesPractice Test On NutritionIvy Yvonne Quinico Malubag100% (1)
- HCW NigeriaDocument12 pagesHCW NigeriaFrancis Njihia KaburuNo ratings yet
- Diabetes - Oral KnowledgeDocument19 pagesDiabetes - Oral KnowledgeKSeegurNo ratings yet
- Rationale: Most Patients Prescribed To Receive Platelet Transfusions Exhibit Moderate ToDocument2 pagesRationale: Most Patients Prescribed To Receive Platelet Transfusions Exhibit Moderate TojoanneNo ratings yet
- Rhopalurus Junceus: and The Treatment of CancerDocument17 pagesRhopalurus Junceus: and The Treatment of CancerAmalia Tri UtamiNo ratings yet
- A Clinical Decision Support Framework ForDocument5 pagesA Clinical Decision Support Framework FordineshshaNo ratings yet
- TTM As5000brochureDocument12 pagesTTM As5000brochureAphichetNo ratings yet
- Toxi TestDocument4 pagesToxi TestFrank NobodNo ratings yet
- Using Lean Six Sigma Techniques To Improve Efficiency in Outpatient Ophthalmology ClinicsDocument9 pagesUsing Lean Six Sigma Techniques To Improve Efficiency in Outpatient Ophthalmology ClinicsMinh Nguyễn Phương HồngNo ratings yet
- Lung Cancer Types & TreatmentsDocument45 pagesLung Cancer Types & TreatmentsHowell Thomas Montilla AlamoNo ratings yet
- Improving Patient Safety in Radiotherapy by Learning From Near Misses, Incidents and ErrorsDocument5 pagesImproving Patient Safety in Radiotherapy by Learning From Near Misses, Incidents and ErrorsrosanaNo ratings yet
- 0315 DVTDocument28 pages0315 DVTEloisa TardioNo ratings yet
- Coombs Test FreddyDocument11 pagesCoombs Test FreddyFreddy Vallejo LeonNo ratings yet
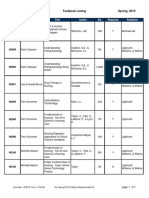
- BFLSON Course Textbook ListingDocument7 pagesBFLSON Course Textbook ListingWina ViqaNo ratings yet