You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Anatomy & Physiology RenalDocument27 pagesAnatomy & Physiology RenalMuchamad Wisuda RiswantoNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Diabetic NephropathyDocument176 pagesDiabetic NephropathyJosé RamírezNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Vasodilators by Hiren PatelDocument28 pagesVasodilators by Hiren PatelHiren_Patel_2427No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Aha Guidelinedriven Management of Hypertension An Evidencebased UpdateDocument56 pagesAha Guidelinedriven Management of Hypertension An Evidencebased UpdateNanda Gopal Reddy AnamNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
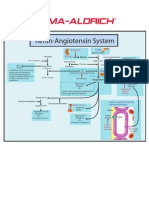
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Stress Response in Critical Illness: Laura Santos, MDDocument9 pagesStress Response in Critical Illness: Laura Santos, MDPutri Wulan SukmawatiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Pediatric Nephrology, 7th EditionDocument65 pagesPediatric Nephrology, 7th EditionDavien Utoyo100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Dr. Hening Tirta Kusumawardani: Mata Kuliah Farmakologi Fakultas Kedokteran Universitas Atmajaya JakartaDocument43 pagesDr. Hening Tirta Kusumawardani: Mata Kuliah Farmakologi Fakultas Kedokteran Universitas Atmajaya JakartaHening Tirta KusumawardaniNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Neurologic Manifestations of Major Electrolyte AbnormalitiesDocument9 pagesNeurologic Manifestations of Major Electrolyte AbnormalitiesMartha OktaviaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- ACE Inhibitors Vs ARBs Is One Class Better For HeaDocument7 pagesACE Inhibitors Vs ARBs Is One Class Better For HeaAfisya sawkiNo ratings yet
- Study of HypertensionDocument44 pagesStudy of HypertensionMathew PiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Clinical Chemistry (Electrolytes)Document27 pagesClinical Chemistry (Electrolytes)2B SALVADOR Jamaica C.No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Unit 06 Blood VesselsDocument101 pagesUnit 06 Blood VesselsJohnykutty JosephNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- S2-OB-Maternal Physio PDFDocument14 pagesS2-OB-Maternal Physio PDFSheena PasionNo ratings yet
- Cardiac Drugs Questions Part IDocument110 pagesCardiac Drugs Questions Part ISanaz Niksefat100% (2)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Unit 1 Study GuideDocument6 pagesUnit 1 Study Guideangieswenson100% (4)
- Hypertensive Heart DiseaseDocument13 pagesHypertensive Heart Diseasemariephynn100% (1)
- 2005 - EMCNA - Disorders of PotassiumDocument25 pages2005 - EMCNA - Disorders of PotassiummagnavlerNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Fluid and Electrolytes - 24 Hours or Less To Absolutely Crush The NCLEX Exam!Document45 pagesFluid and Electrolytes - 24 Hours or Less To Absolutely Crush The NCLEX Exam!KingBlack Canarsie100% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Thesis HSF 2011 Moholisa RetsilisitsoeDocument121 pagesThesis HSF 2011 Moholisa RetsilisitsoeProudAfurakanNo ratings yet
- Chapter 6 - Body Fluids, Water-Salt Balance RP1 PDFDocument77 pagesChapter 6 - Body Fluids, Water-Salt Balance RP1 PDFpizzaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Essential HPNDocument15 pagesEssential HPNchat_killah22No ratings yet
- Fluid and Electrolyte McqsDocument21 pagesFluid and Electrolyte McqsRama Mohan MV93% (42)
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4Document4 pagesBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4ravi2likeNo ratings yet
- Endocrine EssentialsDocument226 pagesEndocrine EssentialsMxt Nút100% (3)
- PBL GM 2Document41 pagesPBL GM 2SleepyHead ˋωˊNo ratings yet
- Devil and Angel in The Renin-Angiotensin System ACE-angiotensin II-AT1 Receptor Axis vs. ACE2-angiotensin - (1-7) - Mas Receptor AxisDocument4 pagesDevil and Angel in The Renin-Angiotensin System ACE-angiotensin II-AT1 Receptor Axis vs. ACE2-angiotensin - (1-7) - Mas Receptor AxisLevente BalázsNo ratings yet
- Formulation and in Vitro Characterization of Time Release Tablets of Propranolol Hydrochloride PDFDocument6 pagesFormulation and in Vitro Characterization of Time Release Tablets of Propranolol Hydrochloride PDFpramod aloorNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Module NCM112 FluidsElectrolytes 2Document58 pagesModule NCM112 FluidsElectrolytes 2bevzie datuNo ratings yet
- Pre-Analytical Consideration and Venipuncture ComplicationsDocument15 pagesPre-Analytical Consideration and Venipuncture ComplicationsJames Anthony ParasNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)