You might also like
- Ankle Fracture EponymsDocument7 pagesAnkle Fracture Eponymsyarianna2No ratings yet
- Hugh Owen Thomas Father of British OrthopaedicsDocument4 pagesHugh Owen Thomas Father of British OrthopaedicschinmayghaisasNo ratings yet
- Rickham's Neonatal SurgeryFrom EverandRickham's Neonatal SurgeryPaul D. LostyNo ratings yet
- Principles and Management of Acute Orthopaedic Trauma: Third EditionFrom EverandPrinciples and Management of Acute Orthopaedic Trauma: Third EditionNo ratings yet
- Odeicia First Aid Kit ProjectDocument25 pagesOdeicia First Aid Kit ProjectDianna LawrenceNo ratings yet
- First Aid and Water SurvivalDocument4 pagesFirst Aid and Water SurvivalRobert MequilaNo ratings yet
- Pecr211 PrelimsDocument5 pagesPecr211 PrelimsPatricia ParicoNo ratings yet
- History OsteomielitisDocument4 pagesHistory OsteomielitisMuhammad Hamka Maha PutraNo ratings yet
- Scurt Istoric FracturiDocument5 pagesScurt Istoric FracturiMusgociu NelaNo ratings yet
- SplintsDocument16 pagesSplintsShini SimonNo ratings yet
- Module Goals: College of Criminal Justice EducationDocument8 pagesModule Goals: College of Criminal Justice EducationAila EchemaneNo ratings yet
- Mitral Valve Disease: Basic Sciences and Current Approaches to ManagementFrom EverandMitral Valve Disease: Basic Sciences and Current Approaches to ManagementNo ratings yet
- Shell-shocked British Army veterans in Ireland, 1918-39: A difficult homecomingFrom EverandShell-shocked British Army veterans in Ireland, 1918-39: A difficult homecomingNo ratings yet
- 7 Tudor Military Surgery and The Management of Sir MartinDocument5 pages7 Tudor Military Surgery and The Management of Sir MartinElizabeth Mautino CaceresNo ratings yet
- Diaphyseal Femur FracturesDocument9 pagesDiaphyseal Femur FracturesSoulmates1No ratings yet
- (316235851) Lisfranc Fracture-Dislocations Powerpoint PresentationDocument40 pages(316235851) Lisfranc Fracture-Dislocations Powerpoint PresentationJustin Michal DassNo ratings yet
- First AidDocument9 pagesFirst AidBradley KenneyNo ratings yet
- The Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingFrom EverandThe Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingJanindra WarusavitarneNo ratings yet
- La Consolacion College Manila: Femoral Neck FractureDocument3 pagesLa Consolacion College Manila: Femoral Neck FractureIvan Liquiran AvenadoNo ratings yet
- Physick to Physiology: Tales from an Oxford Life in MedicineFrom EverandPhysick to Physiology: Tales from an Oxford Life in MedicineNo ratings yet
- Proximal Hamstring Tears: From Endoscopic Repair to Open ReconstructionFrom EverandProximal Hamstring Tears: From Endoscopic Repair to Open ReconstructionThomas YoumNo ratings yet
- Healing by Manipulation - (Bone-Setting) - Jones, J. Henry - 1926 - London - Watts - Anna's ArchiveDocument92 pagesHealing by Manipulation - (Bone-Setting) - Jones, J. Henry - 1926 - London - Watts - Anna's Archivedarksilver.wasfoundbynewtNo ratings yet
- The Accidental Scientist: The Role of Chance and Luck in Scientific DiscoveryFrom EverandThe Accidental Scientist: The Role of Chance and Luck in Scientific DiscoveryNo ratings yet
- Craniosacral Therapy (PDFDrive)Document150 pagesCraniosacral Therapy (PDFDrive)Edina Schlenk-MarkóNo ratings yet
- From Hiroshima to Fukushima to You: A Primer on Radiation and HealthFrom EverandFrom Hiroshima to Fukushima to You: A Primer on Radiation and HealthNo ratings yet
- Salter Textbook of Disorders andDocument729 pagesSalter Textbook of Disorders andGun Gun GunawanNo ratings yet
- Kenneth J. Koval, Joseph D. Zuckerman Auth. Hip Fractures A Practical Guide To ManagementDocument340 pagesKenneth J. Koval, Joseph D. Zuckerman Auth. Hip Fractures A Practical Guide To ManagementWisnu Surya Wardhana100% (2)
- The Principles and Practice of Human PhysiologyFrom EverandThe Principles and Practice of Human PhysiologyO. G. EdholmNo ratings yet
- Veterinary pioneer Apsirtos and his contributions to early veterinary medicineDocument44 pagesVeterinary pioneer Apsirtos and his contributions to early veterinary medicinerogonpouNo ratings yet
- Article - The Mother of NursingDocument3 pagesArticle - The Mother of NursingSilvi SalsabilaNo ratings yet
- The Bankart RepairDocument8 pagesThe Bankart RepairphantomkatalynNo ratings yet
- Emile LetournelDocument4 pagesEmile LetournelMohan DesaiNo ratings yet
- 019 Foot and Ankle ClassificationsDocument13 pages019 Foot and Ankle ClassificationsOh Deh100% (1)
- Traction and Orthopaedic AppliancesDocument1 pageTraction and Orthopaedic Appliancesmanmohansai bacheNo ratings yet
- Orthopaedic Traction TechniquesDocument38 pagesOrthopaedic Traction TechniquesNurul Fitrawati RidwanNo ratings yet
- Immobilization ExtricationDocument75 pagesImmobilization ExtricationJohn Britto100% (3)
- First Aid Procedures for Common Shipboard InjuriesDocument21 pagesFirst Aid Procedures for Common Shipboard InjuriesAzter ReezeNo ratings yet
- Emergency Trauma Care: ATLS: January 2011Document5 pagesEmergency Trauma Care: ATLS: January 2011puaanNo ratings yet
- Self Assessment in Musculoskeletal Pathology X-raysFrom EverandSelf Assessment in Musculoskeletal Pathology X-raysRating: 5 out of 5 stars5/5 (2)
- Bodysnatchers to Livesavers: Three Centuries of Medicine in EdinburghFrom EverandBodysnatchers to Livesavers: Three Centuries of Medicine in EdinburghNo ratings yet
- Do Not Give Up Your Favorite Sport Because Of Joint Sprain !From EverandDo Not Give Up Your Favorite Sport Because Of Joint Sprain !No ratings yet
- Damage Control in Trauma Care: An Evolving Comprehensive Team ApproachFrom EverandDamage Control in Trauma Care: An Evolving Comprehensive Team ApproachJuan DuchesneNo ratings yet
- Ranawat Controlling Pain After Total Hip and Knee SurgeryDocument6 pagesRanawat Controlling Pain After Total Hip and Knee SurgeryPriyank GuptaNo ratings yet
- Local Infiltration Analgesia For SurgeryDocument68 pagesLocal Infiltration Analgesia For SurgeryPriyank GuptaNo ratings yet
- Atrocity Delhi Medical Act PDFDocument7 pagesAtrocity Delhi Medical Act PDFPriyank GuptaNo ratings yet
- Foreign Fellowship of Ioa, Guideline & Selection Criteria For 2o16Document10 pagesForeign Fellowship of Ioa, Guideline & Selection Criteria For 2o16Priyank GuptaNo ratings yet
- Operation Theatre GuidelinesDocument5 pagesOperation Theatre Guidelines21jouhar86% (7)
- 3 Renal BiopsyDocument9 pages3 Renal BiopsyPriyank GuptaNo ratings yet
- Revised Reimbursement Form 2004Document2 pagesRevised Reimbursement Form 2004Priyank GuptaNo ratings yet
- Pre Emptive Analgesia PDFDocument7 pagesPre Emptive Analgesia PDFPriyank GuptaNo ratings yet
- Residency Scheme PDFDocument15 pagesResidency Scheme PDFPriyank Gupta100% (2)
- Asian Paints Book of Colours 2016 Guide to Home Decor TrendsDocument148 pagesAsian Paints Book of Colours 2016 Guide to Home Decor TrendssandeepNo ratings yet
- Percutaneous Renal Biopsy: Louis-Philippe Laurin, Alain Bonnardeaux, Michel Dubé and Martine LeblancDocument15 pagesPercutaneous Renal Biopsy: Louis-Philippe Laurin, Alain Bonnardeaux, Michel Dubé and Martine LeblancShams RehanNo ratings yet
- Renal BiopsyDocument19 pagesRenal BiopsyPriyank GuptaNo ratings yet
- How to Choose Best Health InsuranceDocument5 pagesHow to Choose Best Health InsurancePriyank GuptaNo ratings yet
- Hematological Changes in Chronic Renal FailureDocument4 pagesHematological Changes in Chronic Renal FailurePriyank GuptaNo ratings yet
- DR Bharat Dave - SpinesurgeryfellowshipDocument2 pagesDR Bharat Dave - SpinesurgeryfellowshipPriyank GuptaNo ratings yet
- Baroda Health T and CDocument4 pagesBaroda Health T and Ctovinny14159No ratings yet
- Prospectus New India Floater Medi ClaimDocument17 pagesProspectus New India Floater Medi ClaimPriyank GuptaNo ratings yet
- IAPM FormDocument1 pageIAPM FormPriyank GuptaNo ratings yet
- LHMCDocument3 pagesLHMCPriyank GuptaNo ratings yet
- Bio FilmDocument2 pagesBio FilmKhushbu AgarwalNo ratings yet
- Immunologic AdjuvantDocument5 pagesImmunologic AdjuvantPriyank GuptaNo ratings yet
- Looking After Your New Knee ReplacementDocument1 pageLooking After Your New Knee ReplacementPriyank GuptaNo ratings yet
- Understanding OsteoporosisDocument6 pagesUnderstanding OsteoporosisPriyank GuptaNo ratings yet
- Seizure Care Plan Epilepsy FoundationDocument2 pagesSeizure Care Plan Epilepsy Foundationheather579No ratings yet
- App j.1 Guided Self Regulation AprilDocument29 pagesApp j.1 Guided Self Regulation Aprilda_reaper_dasNo ratings yet
- First Aid Lecture NotesDocument6 pagesFirst Aid Lecture NotesBES BEBENo ratings yet
- First Aid, CPR and Aed-AhaDocument1 pageFirst Aid, CPR and Aed-AhaBenaoumeur FNo ratings yet
- Frist Aid Scenario LibraryDocument9 pagesFrist Aid Scenario LibrarySamuelLiewNo ratings yet
- Hse Requirement: Specification FORDocument28 pagesHse Requirement: Specification FORNizar EnnettaNo ratings yet
- Mapeh-Whlp 4 HealthDocument4 pagesMapeh-Whlp 4 Healthwarren bernardoNo ratings yet
- VAMA Poster DefinitivoDocument1 pageVAMA Poster Definitivocedivadenia8084No ratings yet
- Construction Health and Safety ManualDocument354 pagesConstruction Health and Safety ManualMahmoud Abdallah100% (6)
- Emergency Cardiovascular CareDocument56 pagesEmergency Cardiovascular CareAdit PradaNaNo ratings yet
- Ink V451-D Videojet: Safety Data SheetDocument11 pagesInk V451-D Videojet: Safety Data Sheetsimohamed alaoui aziziNo ratings yet
- Acls Algorithms 2021 ChecklistDocument1 pageAcls Algorithms 2021 ChecklistpepNo ratings yet
- Raviebel Events Lleno Bsoa-3aDocument62 pagesRaviebel Events Lleno Bsoa-3aMariz CinconiegueNo ratings yet
- Maintain First Aid KitsDocument3 pagesMaintain First Aid KitsMarshal OctavianusNo ratings yet
- Rescue Confined WorkersDocument5 pagesRescue Confined WorkersOlaniyi AdewaleNo ratings yet
- Emergency Action Plan TEMP1 - 16Document17 pagesEmergency Action Plan TEMP1 - 16Kim ClaresseNo ratings yet
- Method StatementDocument20 pagesMethod StatementCharles IkenyeNo ratings yet
- 0779 NATO SOF Medical Standards and Training 2009Document78 pages0779 NATO SOF Medical Standards and Training 2009freemedicNo ratings yet
- Q2 DLL SCIENCE COMPLETE QUARTER 2 Inkay PeraltaDocument24 pagesQ2 DLL SCIENCE COMPLETE QUARTER 2 Inkay PeraltaGlen GorgonioNo ratings yet
- Emergency First Aid GuideDocument21 pagesEmergency First Aid GuideJhelene AlyzzaNo ratings yet
- CV for Medical Consultant RoleDocument6 pagesCV for Medical Consultant RoleAlvi MirzaNo ratings yet
- SPM English Sample Essays Based On The Important TopicsDocument15 pagesSPM English Sample Essays Based On The Important TopicsElisha Kirubaraj100% (2)
- BLS MCQDocument8 pagesBLS MCQAmit BhowmikNo ratings yet
- Demo Lesson Plan in MusicDocument3 pagesDemo Lesson Plan in MusicAjarn ShenNo ratings yet
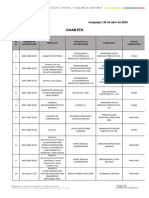
- Guantes: ITE M Número de Autorización Producto Titular de La Autorización Fabricante País de FabricaciónDocument2 pagesGuantes: ITE M Número de Autorización Producto Titular de La Autorización Fabricante País de FabricaciónAdrian AstorgaNo ratings yet
- Checklist Adult CPR OLFU 2022Document2 pagesChecklist Adult CPR OLFU 2022ANGELICA MACASO100% (1)
- First Aid Literature ReviewDocument8 pagesFirst Aid Literature Reviewaflsuhohq100% (1)
- First Aid Basics Study Guide (AutoRecovered)Document4 pagesFirst Aid Basics Study Guide (AutoRecovered)Reuben VarnerNo ratings yet
- Material Safety Data SheetDocument8 pagesMaterial Safety Data SheetAbdelrhman AlaaNo ratings yet
- Caregiving NC IIDocument109 pagesCaregiving NC IITyco Mac100% (1)