You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Position PaperDocument16 pagesPosition PaperMathew McCarthyNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Cir 0000000000000628Document101 pagesCir 0000000000000628Diana AngelesNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Cir 0000000000000628Document101 pagesCir 0000000000000628Diana AngelesNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Cir 0000000000000628Document101 pagesCir 0000000000000628Diana AngelesNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Cir 0000000000000628Document101 pagesCir 0000000000000628Diana AngelesNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Thalassemias and Hemolytic AnemiasDocument43 pagesThe Thalassemias and Hemolytic AnemiasAnonymous elq7jZiSNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- MRCP Recalls May 2014Document15 pagesMRCP Recalls May 2014sohailsu100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Past Paper Questions and AnswersDocument61 pagesPast Paper Questions and AnswerssophiaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- MCQ For University Exam Chapter-Wise: For More Join Us On TelegramDocument6 pagesMCQ For University Exam Chapter-Wise: For More Join Us On TelegramDrug ViralNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Integumentary 2Document13 pagesIntegumentary 2api-302885118No ratings yet
- Blood GroupDocument12 pagesBlood Groupalive computerNo ratings yet
- Cancer Detection by GraphologyDocument5 pagesCancer Detection by GraphologyEndy Mulio100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Protein Structure Powerpoint Presentation Newest Pink and PurpleDocument21 pagesProtein Structure Powerpoint Presentation Newest Pink and Purpleapi-281150432No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- PCR 5 Lab SetupDocument22 pagesPCR 5 Lab Setupptz1965No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- 1.1 Fields and Careers in BiologyDocument5 pages1.1 Fields and Careers in BiologyFHATIN AMIRA BINTI MUSA MoeNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Krizia Joy Borromeo-Galve, MD: Bulacan Medical Center, Department of PediatricsDocument84 pagesKrizia Joy Borromeo-Galve, MD: Bulacan Medical Center, Department of PediatricsTara Oliveros Dela CruzNo ratings yet
- Your Health Today Choices in A Changing Society 5th Edition Teague Test BankDocument29 pagesYour Health Today Choices in A Changing Society 5th Edition Teague Test Banktaylorruiznqfpogxske100% (17)
- Tumor Markers in Common UseDocument10 pagesTumor Markers in Common Usethoai doan vanNo ratings yet
- Calbiochem InhibitorsDocument124 pagesCalbiochem InhibitorsChazMarloweNo ratings yet
- Spatial Transcriptomics Reveals Distinct and Conserved Tumor Core and Edge Architectures That Predict Survival and Targeted Therapy ResponseDocument61 pagesSpatial Transcriptomics Reveals Distinct and Conserved Tumor Core and Edge Architectures That Predict Survival and Targeted Therapy Response戴义宾No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Seizure Disorders: Musupila.M DCM, Adgm, BSC Cs (Unza) 6 November 2019Document26 pagesSeizure Disorders: Musupila.M DCM, Adgm, BSC Cs (Unza) 6 November 2019Emmanuel MukukaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Excretion and HomeostasisDocument31 pagesExcretion and HomeostasiscsamarinaNo ratings yet
- PHILIPPINES Asthma Consensus Guidelines 2009Document134 pagesPHILIPPINES Asthma Consensus Guidelines 2009Sirias_black50% (2)
- Cells of The Immune SystemDocument38 pagesCells of The Immune SystemprabuNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- About The Measure Domain MeasureDocument3 pagesAbout The Measure Domain MeasureMaríaA.SerranoNo ratings yet
- Epidemiological Trends in Skin Mycoses Worldwide: Blanka Havlickova, Viktor A. Czaika and Markus FriedrichDocument14 pagesEpidemiological Trends in Skin Mycoses Worldwide: Blanka Havlickova, Viktor A. Czaika and Markus FriedrichRS Tk IV PekanbaruNo ratings yet
- Improving Eyesight With Red Light TherapyDocument23 pagesImproving Eyesight With Red Light TherapyMark Sloan100% (8)
- Efflux-Mediated Antimicrobial Resistance in Bacteria - Mechanisms, Regulation and Clinical Implications-ADIS (2016)Document850 pagesEfflux-Mediated Antimicrobial Resistance in Bacteria - Mechanisms, Regulation and Clinical Implications-ADIS (2016)jenny joseNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- 6101 01 MSC 20080611Document17 pages6101 01 MSC 20080611sg noteNo ratings yet
- In2Med HaematologyDocument30 pagesIn2Med Haematologye148659No ratings yet
- Rheumatoid ArthritisDocument38 pagesRheumatoid ArthritisOlga GoryachevaNo ratings yet
- Hepatitis C Virus Encoded Antigen DetectionDocument25 pagesHepatitis C Virus Encoded Antigen DetectionPrasanth GovindanNo ratings yet
- Causes of MiscarriageDocument7 pagesCauses of MiscarriageClaire Nimor VentulanNo ratings yet
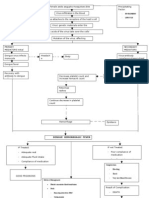
- Pathophysio DHF EDITEDDocument3 pagesPathophysio DHF EDITEDricmichael100% (1)
- Pancreas Anatomy and PhysiologyDocument34 pagesPancreas Anatomy and PhysiologySourabh MishraNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)