You might also like
- Ecthyma Contagiosum (Human Orf)Document2 pagesEcthyma Contagiosum (Human Orf)Deba P SarmaNo ratings yet
- Multiple Dermatofibromas in An Adult FemaleDocument3 pagesMultiple Dermatofibromas in An Adult FemaleDeba P SarmaNo ratings yet
- Case Report: Xanthoma Disseminatum With Tumor-Like Lesion On FaceDocument5 pagesCase Report: Xanthoma Disseminatum With Tumor-Like Lesion On FaceAgus SyaifudinNo ratings yet
- Title of The LecDocument22 pagesTitle of The LecWeird BoiNo ratings yet
- Papular UrticariaDocument10 pagesPapular UrticariaNuri Sakina SuhartoNo ratings yet
- Tinea Capitis EmedicineDocument16 pagesTinea Capitis EmedicineIkram IkramNo ratings yet
- TranslateDocument67 pagesTranslatesriwahyuniNo ratings yet
- Fungal Mycosis and Other InfectionsDocument34 pagesFungal Mycosis and Other InfectionsRajeev PotadarNo ratings yet
- Chromoblastomycosis: Differential DiagnosesDocument4 pagesChromoblastomycosis: Differential DiagnosesPranab ChatterjeeNo ratings yet
- Evaluation of Culture Media For The Rapid Isolation of DermatophytesDocument4 pagesEvaluation of Culture Media For The Rapid Isolation of DermatophytesIOSRjournalNo ratings yet
- Fde CedDocument2 pagesFde CedmdpavlovicNo ratings yet
- Pityriasis Versicolor Definition and NomenclatureDocument8 pagesPityriasis Versicolor Definition and NomenclatureintanphNo ratings yet
- Pityriasis Alba: A Condition With Possibly Multiple EtiologiesDocument2 pagesPityriasis Alba: A Condition With Possibly Multiple EtiologiesAndana Haris R.No ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument33 pagesWorld's Largest Science, Technology & Medicine Open Access Book Publisherlenn chandNo ratings yet
- 1 Gram Positive Bacterial InfectionDocument87 pages1 Gram Positive Bacterial InfectionCoy NuñezNo ratings yet
- Superficial Fungal Infections: Auroba K. Abbas, PH.D., Zahraa A. Mohammed, M.SC., Imad S. Mahmoud, PH.DDocument3 pagesSuperficial Fungal Infections: Auroba K. Abbas, PH.D., Zahraa A. Mohammed, M.SC., Imad S. Mahmoud, PH.DAnonymous zNUqQaNo ratings yet
- Discoid Lupus Erythematosus (DLE) in A Spitz DogDocument3 pagesDiscoid Lupus Erythematosus (DLE) in A Spitz DogPatrícia StancuNo ratings yet
- Bizkova 2009Document8 pagesBizkova 2009mario256No ratings yet
- A Study of Tinea Capitis in ChildrenDocument4 pagesA Study of Tinea Capitis in ChildrenTantriSaptennoPattiradjawaneNo ratings yet
- Fungal InfectionsDocument29 pagesFungal InfectionsKaran MassNo ratings yet
- Medical MycologyDocument14 pagesMedical Mycologyhawkar omerNo ratings yet
- Lapkas Tinea Kapitis Hay2016Document7 pagesLapkas Tinea Kapitis Hay2016Anonymous ykXICaJRUNo ratings yet
- Tinea Capitis Current StatusDocument7 pagesTinea Capitis Current StatusIcutNo ratings yet
- Sysytemic and Opp. MycosisDocument107 pagesSysytemic and Opp. MycosisPrincewill SeiyefaNo ratings yet
- Intertegumentary SystemDocument5 pagesIntertegumentary SystemRoxana AnaNo ratings yet
- 14.PhotoDermDiagnosis Keratotic Papules Over Chest and BackDocument3 pages14.PhotoDermDiagnosis Keratotic Papules Over Chest and BackDwi Tantri SPNo ratings yet
- Pi Is 0190962208009328Document2 pagesPi Is 0190962208009328Nabhya MaheshwariNo ratings yet
- Fungi & Systemic MycosesDocument42 pagesFungi & Systemic MycosesariffdrNo ratings yet
- Demodex Follicullorum Mimicking Fungal Infection A Case ReportDocument2 pagesDemodex Follicullorum Mimicking Fungal Infection A Case ReportAnonymous V5l8nmcSxb100% (1)
- Hongos PerroDocument4 pagesHongos PerroHelen Dellepiane GilNo ratings yet
- AD1110894Document5 pagesAD1110894dhawalduvey95No ratings yet
- Bacterial Skin Infections - Course VIIIDocument37 pagesBacterial Skin Infections - Course VIIIAngelie PedregosaNo ratings yet
- Cutaneous GranulomasDocument2 pagesCutaneous GranulomasloreagubenjiNo ratings yet
- Staphylococcus Epidermidis Research PaperDocument6 pagesStaphylococcus Epidermidis Research Papergw155nah100% (1)
- Demodex Mites - Commensals, Parasites or Mutualistic Organisms?Document3 pagesDemodex Mites - Commensals, Parasites or Mutualistic Organisms?SMA Negeri 1 SedayuNo ratings yet
- Tinea CapitisDocument7 pagesTinea Capitismufidah nurfajNo ratings yet
- Milia PaperDocument14 pagesMilia PaperWito Eka PutraNo ratings yet
- Diffuse Lepromatous Leprosy in An Hiv-Positive PatientDocument7 pagesDiffuse Lepromatous Leprosy in An Hiv-Positive PatientIJAR JOURNALNo ratings yet
- Ebook Dermatology Secrets PDF Full Chapter PDFDocument67 pagesEbook Dermatology Secrets PDF Full Chapter PDFroy.hausler873100% (25)
- Acne and Bacteria Research PaperDocument7 pagesAcne and Bacteria Research Paperqwmojqund100% (1)
- DemodexDocument5 pagesDemodexmigas1996No ratings yet
- Dermatophytosis: LectureDocument35 pagesDermatophytosis: LectureGideon MukalaziNo ratings yet
- Exfoliative DermatitisDocument7 pagesExfoliative DermatitisRidyah Ning TyasNo ratings yet
- Gray Patch Tinea Capitis Caused by Microsporum Canis PDFDocument4 pagesGray Patch Tinea Capitis Caused by Microsporum Canis PDFAnonymous hxXpvZdZNo ratings yet
- Therapeutic Hotline: Tinea Profunda of The Genital Area. Successful Treatment of A Rare Skin DiseaseDocument3 pagesTherapeutic Hotline: Tinea Profunda of The Genital Area. Successful Treatment of A Rare Skin Diseasesoekarnohatta94No ratings yet
- Mycosis Fungoides and Dubreuilhs Melanoma: An Unusual AssociationDocument4 pagesMycosis Fungoides and Dubreuilhs Melanoma: An Unusual AssociationIJAR JOURNALNo ratings yet
- Tinea Capitis Current Status JurnalDocument8 pagesTinea Capitis Current Status Jurnal18310008 ALVIN ANDRIAN SUSANTONo ratings yet
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDocument7 pagesScabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewNovita WulandariNo ratings yet
- What Is The Importance of Demodex Folliculorum in Behcet DiseaseDocument5 pagesWhat Is The Importance of Demodex Folliculorum in Behcet DiseaseRoxana SurliuNo ratings yet
- Tinea Capitis in AdultsDocument7 pagesTinea Capitis in Adultsdimasarya671No ratings yet
- Staphylococci. Bacterial Pyoderma Is UsuallyDocument15 pagesStaphylococci. Bacterial Pyoderma Is UsuallyastricaturutamiNo ratings yet
- (2017) BELOUSOVA, Irena E. Mycosis Fungoides Manifesting As Giant Cell Lichenoid DermatitisDocument3 pages(2017) BELOUSOVA, Irena E. Mycosis Fungoides Manifesting As Giant Cell Lichenoid DermatitisCassandra VérasNo ratings yet
- Dandruff PDFDocument8 pagesDandruff PDFArthur ChietraNo ratings yet
- Scabies and Pediculosis: Neglected Diseases To Highlight: Article Published Online: 1 February 2012Document2 pagesScabies and Pediculosis: Neglected Diseases To Highlight: Article Published Online: 1 February 2012Anonymous TVwR0FNo ratings yet
- E Tra: Diagnosis and Management of Cutaneous Tinea InfectionsDocument8 pagesE Tra: Diagnosis and Management of Cutaneous Tinea InfectionsFuad hadyanNo ratings yet
- Cutaneous Lesions of The Canine ScrotumDocument14 pagesCutaneous Lesions of The Canine ScrotumLuciana Diegues100% (1)
- The Journal of Rheumatology Volume 94, No.: The Microbiome in Psoriasis and Psoriatic Arthritis: The Skin PerspectiveDocument3 pagesThe Journal of Rheumatology Volume 94, No.: The Microbiome in Psoriasis and Psoriatic Arthritis: The Skin PerspectivelizasilvianaNo ratings yet
- Cutaneous Lymphomas: Unusual Cases 3From EverandCutaneous Lymphomas: Unusual Cases 3Oleg E. AkilovNo ratings yet
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaNo ratings yet
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaNo ratings yet
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaNo ratings yet
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNo ratings yet
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaNo ratings yet
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaNo ratings yet
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNo ratings yet
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaNo ratings yet
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNo ratings yet
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNo ratings yet
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNo ratings yet
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNo ratings yet
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaNo ratings yet
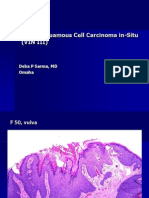
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNo ratings yet
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNo ratings yet
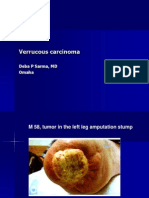
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNo ratings yet
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaNo ratings yet
- Learning Information Booklet Ici London Underground ModuleDocument20 pagesLearning Information Booklet Ici London Underground ModuletiberiuNo ratings yet
- Sindrome de ReyeDocument5 pagesSindrome de ReyecdsaludNo ratings yet
- Universiti Pendidikan Sultan Loris: IiiiiDocument13 pagesUniversiti Pendidikan Sultan Loris: IiiiiSarathy Hari KumarNo ratings yet
- Microorganisms in Kitchen SpongesDocument6 pagesMicroorganisms in Kitchen SpongesYami SainzNo ratings yet
- AFFIDAVIT OF UNDERTAKING TIMO Coach As AccompanyingDocument1 pageAFFIDAVIT OF UNDERTAKING TIMO Coach As AccompanyingDisco CreeperNo ratings yet
- Reportorial RubricDocument3 pagesReportorial RubricDerrick HartNo ratings yet
- Mosaic Laws For Good HealthDocument1 pageMosaic Laws For Good Healthgjbrown888No ratings yet
- MalariaDocument4 pagesMalarianafrabNo ratings yet
- Science Investigatory ProjectDocument2 pagesScience Investigatory ProjectYra Louisse TaromaNo ratings yet
- Clostridium Botulinum - Ecology and Control in Foods (1993)Document762 pagesClostridium Botulinum - Ecology and Control in Foods (1993)RhynoHD100% (1)
- DR Kamal G IshakDocument2 pagesDR Kamal G Ishakmike116No ratings yet
- New PMDC Neb Format 2011Document28 pagesNew PMDC Neb Format 2011AliHazratNo ratings yet
- Medical English Vocabulary: Nurses and Medical ProfessionalsDocument15 pagesMedical English Vocabulary: Nurses and Medical ProfessionalsEchan MitnickNo ratings yet
- Anatomy of Human EarDocument5 pagesAnatomy of Human EarSharanz Twentyfour SevenNo ratings yet
- Standard Surgical Attire Surgical ScrubDocument20 pagesStandard Surgical Attire Surgical ScrubzekkipianoNo ratings yet
- Aravind's Atlas of Fungal Corneal Ulcers - Clinical Features and Laboratory Identification MethodsDocument161 pagesAravind's Atlas of Fungal Corneal Ulcers - Clinical Features and Laboratory Identification MethodsSurendar KesavanNo ratings yet
- Mauritius Government GazetteDocument2 pagesMauritius Government GazetteAmrit ChutoorgoonNo ratings yet
- HEPATITEDocument49 pagesHEPATITEAeron TamayoNo ratings yet
- Medicinal and Magical Herbs of Medieval EuropeDocument13 pagesMedicinal and Magical Herbs of Medieval EuropePagan Hare100% (1)
- Kyasanur Forest Disease PDFDocument10 pagesKyasanur Forest Disease PDFKarthik SNo ratings yet
- Protimo Antimicrobial Agent Introduction-2013-08-08 PDFDocument27 pagesProtimo Antimicrobial Agent Introduction-2013-08-08 PDF連宗興No ratings yet
- Interpretation of Life ExpectancyDocument6 pagesInterpretation of Life ExpectancyChristopher PrestonNo ratings yet
- Pelvic Crossed SyndromeDocument2 pagesPelvic Crossed SyndromeSimo AsterNo ratings yet
- Medical Virology, IntroductionMedical VirologyDocument88 pagesMedical Virology, IntroductionMedical Virologytummalapalli venkateswara rao100% (4)
- NCP To NG PneumoniaDocument3 pagesNCP To NG PneumoniaGlenn Asuncion PagaduanNo ratings yet
- ARDS PathophysiologyDocument2 pagesARDS PathophysiologyIntanAgustiFernandesNo ratings yet
- New Drug 2010 Upto Aug 2010Document15 pagesNew Drug 2010 Upto Aug 2010NAVNEET BAGGANo ratings yet
- Reserch Impo 4Document25 pagesReserch Impo 4Ceej Bahian SacabinNo ratings yet
- Herpes Simplex & Molluscum ContagiosumDocument24 pagesHerpes Simplex & Molluscum Contagiosumbasic100% (2)
- Aortic Valve DiseaseDocument25 pagesAortic Valve Diseasesagungw93No ratings yet