You might also like
- DUP436 Big Pharma2 PDFDocument16 pagesDUP436 Big Pharma2 PDFHITESH MAKHIJANo ratings yet
- DUP436 Big Pharma2 PDFDocument16 pagesDUP436 Big Pharma2 PDFJose CMNo ratings yet
- Physician Leaders of Medical Groups Face Increasing ChallengesDocument6 pagesPhysician Leaders of Medical Groups Face Increasing ChallengesAli RajaNo ratings yet
- Medicare Prescription Drugs: Medical Necessity Meets Fiscal Insanity Cato Briefing Paper No. 91Document12 pagesMedicare Prescription Drugs: Medical Necessity Meets Fiscal Insanity Cato Briefing Paper No. 91Cato InstituteNo ratings yet
- Reducing Administrative Costs and Improving The Health Care SystemDocument4 pagesReducing Administrative Costs and Improving The Health Care Systemrongse@gmail.comNo ratings yet
- (2-12) What Is Life CostDocument5 pages(2-12) What Is Life Cost陳銑鈞No ratings yet
- Health Care Regulation: A $169 Billion Hidden Tax Cato Policy Analysis No. 527Document32 pagesHealth Care Regulation: A $169 Billion Hidden Tax Cato Policy Analysis No. 527Cato Institute100% (3)
- Porter y Kapplan (2011)Document18 pagesPorter y Kapplan (2011)ANA MARIA RIOSNo ratings yet
- Value and Payment in Sleep Medicine JCSM 2018Document4 pagesValue and Payment in Sleep Medicine JCSM 2018cjbae22No ratings yet
- Robert BerensonDocument29 pagesRobert Berensonapi-239368329No ratings yet
- The Art of the Heal: A Health Executive’s Guide to Innovating HospitalsFrom EverandThe Art of the Heal: A Health Executive’s Guide to Innovating HospitalsNo ratings yet
- 7 Market Access Trends For 2027Document14 pages7 Market Access Trends For 2027Anshuman BudhirajaNo ratings yet
- The Impact of COVID-19 On Small Business Outcomes and ExpectationsDocument3 pagesThe Impact of COVID-19 On Small Business Outcomes and ExpectationsGLADYS MARINA NUÑEZ QUISPENo ratings yet
- MMMMDocument3 pagesMMMMMaria Galla'No ratings yet
- Banks & Health Players CollaborateDocument10 pagesBanks & Health Players Collaboratejliebie83No ratings yet
- Health Care Inflation PDFDocument4 pagesHealth Care Inflation PDFsherifNo ratings yet
- Research Paper in Health EconomicsDocument6 pagesResearch Paper in Health Economicscaqllprhf100% (1)
- Health Care Price Data WSJDocument3 pagesHealth Care Price Data WSJbob smithNo ratings yet
- Labor Markets and Health Care Refor M: New Results: Executive SummaryDocument6 pagesLabor Markets and Health Care Refor M: New Results: Executive Summaryapi-27836025No ratings yet
- Payers & Providers - Issue of May 13, 2010Document7 pagesPayers & Providers - Issue of May 13, 2010PayersandProvidersNo ratings yet
- Financial Environment of Health Care OrganizationsDocument40 pagesFinancial Environment of Health Care OrganizationsNeicy Wilson100% (1)
- Policy Brief 3 ThelenDocument16 pagesPolicy Brief 3 ThelenCarol ThelenNo ratings yet
- Controlling Health Care CostsDocument3 pagesControlling Health Care CostsAthanassios VozikisNo ratings yet
- Home Care Position Paper 4 5 111 PDFDocument20 pagesHome Care Position Paper 4 5 111 PDFRichard HutasoitNo ratings yet
- HealthLaw 02springDocument4 pagesHealthLaw 02springflastergreenbergNo ratings yet
- US Deloittereview Im Okay Youre Okay But Will We Be All Right Jul11Document13 pagesUS Deloittereview Im Okay Youre Okay But Will We Be All Right Jul11Kedar KelkarNo ratings yet
- Health Plan Price TransparencyDocument16 pagesHealth Plan Price TransparencyMartha Bebinger100% (1)
- Expect The UnexpectedDocument13 pagesExpect The UnexpectedPeter ArmaosNo ratings yet
- A Role For EntrepreneursDocument5 pagesA Role For EntrepreneursDelia NiculaNo ratings yet
- Thinking Outside The Box Moving The Respiratory Care ProfessionDocument9 pagesThinking Outside The Box Moving The Respiratory Care Professionnicomat85No ratings yet
- Payers & Providers: Californians Shirking Regular CareDocument6 pagesPayers & Providers: Californians Shirking Regular CarepayersprovidersNo ratings yet
- Chapter 2 - Tools of Positive Analysis Brief Outline: Part 1 - Getting StartedDocument3 pagesChapter 2 - Tools of Positive Analysis Brief Outline: Part 1 - Getting StartedTâm Trần Thị MinhNo ratings yet
- PWC Hri Top Healthcare Issues 2017Document23 pagesPWC Hri Top Healthcare Issues 2017devanNo ratings yet
- The Business of Medicine in The Era of COVID-19Document2 pagesThe Business of Medicine in The Era of COVID-19oke dmmNo ratings yet
- COVID 19 and Commercial PharmaceuticalsDocument13 pagesCOVID 19 and Commercial Pharmaceuticalsrocket skyNo ratings yet
- Contemporary Socio-Economic Issues Facing Filipino EntrepreneursDocument7 pagesContemporary Socio-Economic Issues Facing Filipino EntrepreneursCarmilleah Freyjah75% (4)
- Journal of Bioequivalence & Bioavailability: The Inevitable Future of Generic Pharma Drugs CompaniesDocument2 pagesJournal of Bioequivalence & Bioavailability: The Inevitable Future of Generic Pharma Drugs CompaniesraviNo ratings yet
- Patient Satisfaction PDFDocument5 pagesPatient Satisfaction PDFBîrlădeanu Ramona ElenaNo ratings yet
- Moody Report On HealthcareDocument6 pagesMoody Report On HealthcareDan TrangNo ratings yet
- Financial Resilience TaskForce Report - 29.10.19Document36 pagesFinancial Resilience TaskForce Report - 29.10.19Mark Anthony KionisalaNo ratings yet
- LWV RecentHealthCareChangesDocument4 pagesLWV RecentHealthCareChangesjrfh50No ratings yet
- Mining for Gold In a Barren Land: Pioneer Accountable Care Organization Potential to Redesign the Healthcare Business Model in a Post-Acute SettingFrom EverandMining for Gold In a Barren Land: Pioneer Accountable Care Organization Potential to Redesign the Healthcare Business Model in a Post-Acute SettingNo ratings yet
- Benefit Incidence Analysis: Policy Research Working Paper 5234Document25 pagesBenefit Incidence Analysis: Policy Research Working Paper 5234C12AYNo ratings yet
- Taxes As Pandemic Controls: Ashley C. Craig University of MichiganDocument24 pagesTaxes As Pandemic Controls: Ashley C. Craig University of MichiganJOENo ratings yet
- Leadership Skills for the New Health Economy a 5Q© ApproachFrom EverandLeadership Skills for the New Health Economy a 5Q© ApproachNo ratings yet
- Fin Plan Rev - 2020 - Fox - Household Finances Financial Planning and COVID 19Document9 pagesFin Plan Rev - 2020 - Fox - Household Finances Financial Planning and COVID 19Nur AlamNo ratings yet
- Health Benefit Satisfaction in The Public and Private Sectors: The Role of Distributive and Procedural JusticeDocument16 pagesHealth Benefit Satisfaction in The Public and Private Sectors: The Role of Distributive and Procedural JusticePedro Alberto Herrera LedesmaNo ratings yet
- Patient-Reported Outcomes - Are They Living Up To Their Potential?Document4 pagesPatient-Reported Outcomes - Are They Living Up To Their Potential?Katerina TsNo ratings yet
- Athens Medical Claims ReengineeringDocument8 pagesAthens Medical Claims ReengineeringmarkbilamouthNo ratings yet
- wk7 DQDocument7 pageswk7 DQharum haiNo ratings yet
- Health CareDocument5 pagesHealth Care6xmarkNo ratings yet
- Paper Cuts: Reducing Health Care Administrative CostsDocument48 pagesPaper Cuts: Reducing Health Care Administrative CostsCenter for American ProgressNo ratings yet
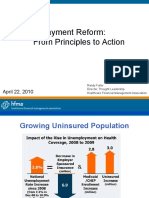
- Payment Reform: From Principles to ActionDocument34 pagesPayment Reform: From Principles to Actionibson045001256No ratings yet
- Elaborating Prioritization in Healthcare Amidst A Global COVID-19 PandemicDocument3 pagesElaborating Prioritization in Healthcare Amidst A Global COVID-19 PandemicInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- SWOTDocument14 pagesSWOTLisaNo ratings yet
- 05 29 Nasi SpeechDocument14 pages05 29 Nasi SpeechLisaNo ratings yet
- Privitization and The Allure of FranchisingDocument26 pagesPrivitization and The Allure of FranchisingZoe KhanNo ratings yet
- Health Car em A Whitepaper 2010Document16 pagesHealth Car em A Whitepaper 2010sunsetstarzNo ratings yet
- Does The Doctor Need A Boss?, Cato Briefing Paper No. 111Document12 pagesDoes The Doctor Need A Boss?, Cato Briefing Paper No. 111Cato InstituteNo ratings yet
- Transparency and The Doctor-Patient Relationship - Rethinking Conflict-of-Interest DisclosuresDocument3 pagesTransparency and The Doctor-Patient Relationship - Rethinking Conflict-of-Interest Disclosurespogesil46No ratings yet
- Selling Primary Care PracticeDocument6 pagesSelling Primary Care PracticeSauer Consulting, LLCNo ratings yet
- A Balanced Approach To Physician CompensationDocument4 pagesA Balanced Approach To Physician CompensationSauer Consulting, LLCNo ratings yet
- CXO Summit 2010 - Partnering Physicians With HospitalsDocument44 pagesCXO Summit 2010 - Partnering Physicians With HospitalsSauer Consulting, LLCNo ratings yet
- Creating Success With IDSDocument2 pagesCreating Success With IDSSauer Consulting, LLCNo ratings yet
- United We Stand: Power Shifts Marginalize Physician Practices Unless We Act and IntegrateDocument6 pagesUnited We Stand: Power Shifts Marginalize Physician Practices Unless We Act and IntegrateSauer Consulting, LLCNo ratings yet
- 2015 International Profiles of Health Care Systems (Commonwealth Fund)Document180 pages2015 International Profiles of Health Care Systems (Commonwealth Fund)anon_348102417No ratings yet
- Cedarbrook Nursing Home Operational Assessment ReportDocument83 pagesCedarbrook Nursing Home Operational Assessment ReportScott OttNo ratings yet
- PTDischarge Planning Reminder FinalDocument2 pagesPTDischarge Planning Reminder Finalbesho 2013No ratings yet
- Telehealth Research and Evaluation Implications For Decision MakersDocument9 pagesTelehealth Research and Evaluation Implications For Decision Makerscharlsandroid01No ratings yet
- Summary Public Finance Chapter 1 16Document17 pagesSummary Public Finance Chapter 1 16Nara Aleesha100% (1)
- Advanstar Biopharm0112Document54 pagesAdvanstar Biopharm0112StrazdasNo ratings yet
- AcronymsDocument153 pagesAcronymsDavid F. Duque G.No ratings yet
- 2023 Medicare KickoffDocument27 pages2023 Medicare KickofflollieNo ratings yet
- Medical Symptoms QuestionnaireDocument29 pagesMedical Symptoms QuestionnaireOlesiaNo ratings yet
- Blueshield Gold Trio HMO 1500:35Document14 pagesBlueshield Gold Trio HMO 1500:35jaroopaitummaiNo ratings yet
- CMS 1450 (UB 04) InstructionsDocument12 pagesCMS 1450 (UB 04) InstructionsKarna Palanivelu67% (3)
- Hye Doun: A Publication of The Armenian Nursing and Rehabilitation Center, Inc., Emerson, NJDocument12 pagesHye Doun: A Publication of The Armenian Nursing and Rehabilitation Center, Inc., Emerson, NJanrcinfoNo ratings yet
- 15 S 16Document23 pages15 S 16Nick ReismanNo ratings yet
- OASIS-E Guidance Manual - 5.16.22Document396 pagesOASIS-E Guidance Manual - 5.16.22mosaNo ratings yet
- Letter To Gilead From AG HealeyDocument5 pagesLetter To Gilead From AG HealeyGintautas DumciusNo ratings yet
- HPA 14 Assignemnt Due November 30thDocument4 pagesHPA 14 Assignemnt Due November 30thcNo ratings yet
- Medicare Marketing GuidelinesDocument119 pagesMedicare Marketing Guidelinesapi-257249241No ratings yet
- Medicare BasicsDocument56 pagesMedicare Basicsapi-239463541No ratings yet
- Social Welfare Position PaperDocument11 pagesSocial Welfare Position Paperapi-617924570No ratings yet
- American Medical Association - ICD-10-CM Documentation_ Essential Charting Guidance to Support Medical Necessity 2019-American Medical Association (2018)Document1,229 pagesAmerican Medical Association - ICD-10-CM Documentation_ Essential Charting Guidance to Support Medical Necessity 2019-American Medical Association (2018)johnharnsberryNo ratings yet
- Draft Ccla Lab Compliance Matrix 3 17 2015 DWTDocument5 pagesDraft Ccla Lab Compliance Matrix 3 17 2015 DWTAmyNo ratings yet
- Evidence-Based Dentistry: EBD and Health Care PlansDocument45 pagesEvidence-Based Dentistry: EBD and Health Care PlansMaha LakshmiNo ratings yet
- Considerations For Group, Concurrent, and Individual TherapyDocument2 pagesConsiderations For Group, Concurrent, and Individual TherapyMysti ReederNo ratings yet
- VP Marketing Bus Dev Strategic Planning International 3 19 PDFDocument9 pagesVP Marketing Bus Dev Strategic Planning International 3 19 PDFcarla singletonNo ratings yet
- Medicare Plus - Family Health Plan - Private - 200k MBLDocument6 pagesMedicare Plus - Family Health Plan - Private - 200k MBLCaindoy ReginielNo ratings yet
- (English) Social Policy - Crash Course Government and Politics #49 (DownSub - Com)Document7 pages(English) Social Policy - Crash Course Government and Politics #49 (DownSub - Com)Ken Brian NasolNo ratings yet
- Harry Dent - RecessionDocument7 pagesHarry Dent - RecessionSue Marks100% (2)
- (English (Auto-Generated) ) Why Innovative Uses of Telehealth Should Be Championed - Christine Zack - TEDxReno (DownSub - Com)Document12 pages(English (Auto-Generated) ) Why Innovative Uses of Telehealth Should Be Championed - Christine Zack - TEDxReno (DownSub - Com)audiNo ratings yet
- Mohammadi Group - Garments ManufacturerDocument39 pagesMohammadi Group - Garments ManufacturerGarmentLearnerNo ratings yet
- Comp 01 Instructor ManualDocument54 pagesComp 01 Instructor ManualP D SpencerNo ratings yet