You might also like
- Center For MedicareDocument1 pageCenter For Medicareapi-25909546No ratings yet
- UntitledDocument2 pagesUntitledapi-25909546No ratings yet
- Summary TablesDocument36 pagesSummary Tablesapi-25909546No ratings yet
- UntitledDocument2 pagesUntitledapi-25909546No ratings yet
- Summary TablesDocument36 pagesSummary Tablesapi-25909546No ratings yet
- UntitledDocument2 pagesUntitledapi-25909546No ratings yet
- ERN10381Document19 pagesERN10381Sarah KliffNo ratings yet
- UntitledDocument2 pagesUntitledapi-25909546No ratings yet
- UntitledDocument2 pagesUntitledapi-25909546No ratings yet
- Commonwealth of Virginia v. Sibelius Et AlDocument42 pagesCommonwealth of Virginia v. Sibelius Et AlDoug MataconisNo ratings yet
- Health Care Ruling by Judge VinsonDocument78 pagesHealth Care Ruling by Judge Vinsond-fbuser-31924476No ratings yet
- GOP Pledge To AmericaDocument21 pagesGOP Pledge To AmericaCBS News57% (7)
- UntitledDocument2 pagesUntitledapi-25909546No ratings yet
- Summary of The Medicare and Medicaid Extenders Act of 2010Document3 pagesSummary of The Medicare and Medicaid Extenders Act of 2010api-25909546No ratings yet
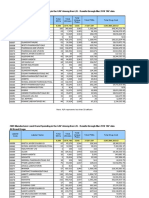
- 2009 Manufacturer-Level Brand Spending in The GAP Among Non-LIS - Results Through Mar 2010 TAP Data All Brand DrugsDocument13 pages2009 Manufacturer-Level Brand Spending in The GAP Among Non-LIS - Results Through Mar 2010 TAP Data All Brand Drugsapi-25909546No ratings yet
- CMSPersonnelAnnouncement10 11 29Document2 pagesCMSPersonnelAnnouncement10 11 29api-25909546No ratings yet
- The Moment of TruthDocument59 pagesThe Moment of TruthAnonymous 4Dry26Y4No ratings yet
- State of Florida v. United States Dept of HHSDocument65 pagesState of Florida v. United States Dept of HHSDoug MataconisNo ratings yet
- CMSDonaldBerwickSFCTestimony10 11 15.10Document16 pagesCMSDonaldBerwickSFCTestimony10 11 15.10api-25909546No ratings yet
- PPTRASummaryFinal10 11 18Document1 pagePPTRASummaryFinal10 11 18api-25909546No ratings yet
- 2009 Manufacturer-Level Brand Spending in The GAP Among Non-LIS - Results Through Mar 2010 TAP Data All Brand DrugsDocument13 pages2009 Manufacturer-Level Brand Spending in The GAP Among Non-LIS - Results Through Mar 2010 TAP Data All Brand Drugsapi-25909546No ratings yet
- IOWAINSCOMM MLRWaiverRequest10 09 21Document2 pagesIOWAINSCOMM MLRWaiverRequest10 09 21api-25909546No ratings yet
- FDACensorCase10 09 29Document2 pagesFDACensorCase10 09 29api-25909546No ratings yet
- A Bill: 111 Congress 2 SDocument3 pagesA Bill: 111 Congress 2 Sapi-25909546No ratings yet
- MedicareSocialSecurityTRUSTEES TREASURYCMSReleases10 08 05Document6 pagesMedicareSocialSecurityTRUSTEES TREASURYCMSReleases10 08 05api-25909546No ratings yet
- Affordable Care Act Update: Implementing Medicare Costs SavingsDocument10 pagesAffordable Care Act Update: Implementing Medicare Costs Savingsapi-25909546No ratings yet
- CMSPOTUSSignsDocFix10 06 25Document1 pageCMSPOTUSSignsDocFix10 06 25api-25909546No ratings yet
- Revised Extenders Doc Fix Substitute Mat 10482Document399 pagesRevised Extenders Doc Fix Substitute Mat 10482api-27836025No ratings yet
- SENATEBaucusSec526AMPIncreasesMT1051210 06 23Document1 pageSENATEBaucusSec526AMPIncreasesMT1051210 06 23api-25909546No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Medicaid Program - A Brief OverviewDocument4 pagesThe Medicaid Program - A Brief Overviewximena.torresNo ratings yet
- Hs 2 Essay1-2Document1 pageHs 2 Essay1-2api-458754298No ratings yet
- Work Plan Office of Inspector General U.S. Department of Health and Human ServicesDocument67 pagesWork Plan Office of Inspector General U.S. Department of Health and Human ServicesSpit FireNo ratings yet
- Nys Medicaid Pre-Adjudication Crosswalk For Health Care ClaimsDocument4 pagesNys Medicaid Pre-Adjudication Crosswalk For Health Care ClaimsTeresaNo ratings yet
- Delmar Gardens of Green Valley 03-09-2018Document10 pagesDelmar Gardens of Green Valley 03-09-2018Scott DavidsonNo ratings yet
- Community Resource List 15-16Document2 pagesCommunity Resource List 15-16Sergio Hidalgo BronfmanNo ratings yet
- WA DSHS Report On Enumclaw Health and Rehab's COVID-19 ProceduresDocument11 pagesWA DSHS Report On Enumclaw Health and Rehab's COVID-19 ProceduresRay StillNo ratings yet
- Modupeore Ajibade Interview AssignmentDocument10 pagesModupeore Ajibade Interview AssignmentBenedict KakaiNo ratings yet
- DDC SVC BRO 0115 Fault CodesDocument16 pagesDDC SVC BRO 0115 Fault CodesAdhem El SayedNo ratings yet
- Matrix - in Home Assessment Info - HUM2012 Humana Brochure - 082712Document2 pagesMatrix - in Home Assessment Info - HUM2012 Humana Brochure - 082712abaker620No ratings yet
- Module 2Document8 pagesModule 2Jeannezelle Anne Mariz GazaNo ratings yet
- Essential Estate Planning DocumentsDocument6 pagesEssential Estate Planning DocumentsTexas Public RadioNo ratings yet
- Joint Communication Bulletin # J429 Terminating Requirement of The LOCUS and CALOCUS 08172022Document1 pageJoint Communication Bulletin # J429 Terminating Requirement of The LOCUS and CALOCUS 08172022Mistor WilliamsNo ratings yet
- CMS K TagsDocument50 pagesCMS K TagsHermes VacaNo ratings yet
- Bemis Healthcare PackagingDocument1 pageBemis Healthcare PackagingJaredNo ratings yet
- Why Coding Is ImportantDocument35 pagesWhy Coding Is ImportantKholylah Afifah Nur RangkutiNo ratings yet
- Utpatient Ospital Ervices: F:/P11/NHI/TRICOMM/AAHCA09 - 001.XMLDocument8 pagesUtpatient Ospital Ervices: F:/P11/NHI/TRICOMM/AAHCA09 - 001.XMLVino DNo ratings yet
- AandDWaiver IdahoDocument175 pagesAandDWaiver IdahoGrammaDestinyNo ratings yet
- White Paper RIS Meaningful Use Guide 201211Document51 pagesWhite Paper RIS Meaningful Use Guide 201211Jose VasquezNo ratings yet
- OneOncology Appoints Dr. John Fox Medical Director For Managed CareDocument2 pagesOneOncology Appoints Dr. John Fox Medical Director For Managed CarePR.comNo ratings yet
- AV Comment Letter - CY 2025 MA Proposed Rule - 1.4 - FinalDocument14 pagesAV Comment Letter - CY 2025 MA Proposed Rule - 1.4 - FinalArnold VenturesNo ratings yet
- Medicare Claims Processing Manual: Chapter 1 - General Billing RequirementsDocument314 pagesMedicare Claims Processing Manual: Chapter 1 - General Billing RequirementsMaurice MarchantNo ratings yet
- Trends and Issues On Family NursingDocument34 pagesTrends and Issues On Family NursingDevita FebyNo ratings yet
- HCAHPS Scores and CommunityDocument11 pagesHCAHPS Scores and CommunityJeff LNo ratings yet
- Cardiology Billing ServicesDocument3 pagesCardiology Billing Servicesnixxe mbsNo ratings yet
- Golden Glades Inspection Report 12/11/2015Document11 pagesGolden Glades Inspection Report 12/11/2015News-PressNo ratings yet
- Certificate of Medical Necessity Dmerc 10.02BDocument2 pagesCertificate of Medical Necessity Dmerc 10.02BjackNo ratings yet
- Death Obituary Cause of Death Ookht PDFDocument4 pagesDeath Obituary Cause of Death Ookht PDFMayerRhodes8No ratings yet
- Comptroller's 2017 Review of TennCare: Memo and ReportDocument11 pagesComptroller's 2017 Review of TennCare: Memo and ReportUSA TODAY NetworkNo ratings yet
- Student Emergency Information Card 2021-2022Document1 pageStudent Emergency Information Card 2021-2022api-291350308No ratings yet