You might also like
- Singapore Dental Claim Form Interactive M003 60E 010115Document5 pagesSingapore Dental Claim Form Interactive M003 60E 010115Nazim SalehNo ratings yet
- AUS Bupa Global Claim Form EN APR21 0028299Document8 pagesAUS Bupa Global Claim Form EN APR21 0028299ALJABERNo ratings yet
- AXA Reimbursement Claim FormDocument2 pagesAXA Reimbursement Claim Formrajkamal eshwarNo ratings yet
- BINS Bupa Global Claim Form en 2005 21089Document8 pagesBINS Bupa Global Claim Form en 2005 21089R.Pearlsis SophiNo ratings yet
- BAH Bupa Global Claim Form EN APR21 0027975Document8 pagesBAH Bupa Global Claim Form EN APR21 0027975ALJABERNo ratings yet
- Claim form submission made simpleDocument7 pagesClaim form submission made simpleEduskill Learning CentreNo ratings yet
- DataLink Claim FormDocument2 pagesDataLink Claim FormAzrul Azuar Azrul Azuar100% (1)
- Allianz claim formDocument2 pagesAllianz claim formCarlo_Sturlese_4203No ratings yet
- Claim Form en Nov 08Document4 pagesClaim Form en Nov 08Juju FernsNo ratings yet
- MS Health Claim FormDocument2 pagesMS Health Claim FormBalaji_Rajaman_2280No ratings yet
- NOW HEALTH Claim - Form - Uae - RsaDocument2 pagesNOW HEALTH Claim - Form - Uae - RsaWilliam IsaacNo ratings yet
- SGP Generic Claim FormDocument5 pagesSGP Generic Claim FormSanny HamdaniNo ratings yet
- Medical Report and ReceiptDocument5 pagesMedical Report and Receiptkumarsam087No ratings yet
- Group Hospital Claim Form GuideDocument5 pagesGroup Hospital Claim Form GuideGelson Herrera0% (5)
- GMHP Claim Form - Online PDFDocument4 pagesGMHP Claim Form - Online PDFSalem AmraneNo ratings yet
- Claim Form GuideDocument2 pagesClaim Form GuideمولديياNo ratings yet
- Application For Chief Minister Relief FundDocument5 pagesApplication For Chief Minister Relief FundVamsi KrishnaNo ratings yet
- Mumbai Claim FormDocument5 pagesMumbai Claim FormsunsangraNo ratings yet
- CLAIM FORM Maternity MEAF RSA 69041 3Document5 pagesCLAIM FORM Maternity MEAF RSA 69041 3Arindam ChangdarNo ratings yet
- AETNADocument5 pagesAETNATRTNo ratings yet
- OVHC Claim Form 102017 PDFDocument3 pagesOVHC Claim Form 102017 PDFtarmudiNo ratings yet
- Ap Chief Minister'S Relief FundDocument6 pagesAp Chief Minister'S Relief Fundiqbal1439988100% (1)
- Claim Form Regency For Expats PDFDocument2 pagesClaim Form Regency For Expats PDFChris DarkNo ratings yet
- BSIB GHS Claim FormDocument3 pagesBSIB GHS Claim FormmuhsinmohammedNo ratings yet
- CMRF Application FormDocument5 pagesCMRF Application FormMohammed AliNo ratings yet
- Claim - Form - 001Document2 pagesClaim - Form - 001nitinmisra77No ratings yet
- REV - Outpatient Claim Form - AIADocument2 pagesREV - Outpatient Claim Form - AIAYen SylvaniNo ratings yet
- Disability Claim Form v3Document7 pagesDisability Claim Form v3arekp28978No ratings yet
- Bupa International Claim Form: 1 Patient'S DetailsDocument4 pagesBupa International Claim Form: 1 Patient'S DetailsRealty SolutionsNo ratings yet
- MaxBupa Pre Auth Claim FormDocument5 pagesMaxBupa Pre Auth Claim FormvineetNo ratings yet
- Hospitalization Reimbursment Claim FormDocument4 pagesHospitalization Reimbursment Claim FormFarhan aliNo ratings yet
- Ahmedabad Claim FormDocument5 pagesAhmedabad Claim FormFirdaus PanthakyNo ratings yet
- Form BUPADocument4 pagesForm BUPAterusunduhNo ratings yet
- Application For Chief Minister Relief FundDocument5 pagesApplication For Chief Minister Relief FundVenkateswarlu ChennaiepalemNo ratings yet
- Domestic Maid Claim FormDocument4 pagesDomestic Maid Claim FormHihiNo ratings yet
- Attending Physician StatementDocument1 pageAttending Physician StatementAnnabeth WatkinsNo ratings yet
- Claim Form Page1 & 2Document2 pagesClaim Form Page1 & 2anwarshahphd2021No ratings yet
- AXA Reimbursement Form ALL enDocument2 pagesAXA Reimbursement Form ALL enReynard Delos SantosNo ratings yet
- Pre Auth Form Revised PDFDocument5 pagesPre Auth Form Revised PDFNILESHNo ratings yet
- NTUC Pa Paid Claim Form (08 2017)Document5 pagesNTUC Pa Paid Claim Form (08 2017)pat5355No ratings yet
- Bupa Global Reimbursement FormDocument5 pagesBupa Global Reimbursement Formshena0% (1)
- Health India TPA - Pre Auth FormDocument5 pagesHealth India TPA - Pre Auth FormBOOKREADER_NOW100% (1)
- Cigna TTK-preauthDocument2 pagesCigna TTK-preauthBOOKREADER_NOWNo ratings yet
- FRM GPPF en 0516Document2 pagesFRM GPPF en 0516Adel NewtonNo ratings yet
- Ap Chief Minister'S Relief Fund: ReimbursementDocument6 pagesAp Chief Minister'S Relief Fund: Reimbursementiqbal1439988No ratings yet
- Hospital Treatment Claim Form DetailsDocument1 pageHospital Treatment Claim Form Detailssachinsaboo3No ratings yet
- Medical Fitness CertificateDocument2 pagesMedical Fitness CertificatePraveen Kumar Madupu100% (1)
- Medical Insurance Claim Form (Corporate)Document3 pagesMedical Insurance Claim Form (Corporate)hari198902234No ratings yet
- Medical Claim - Doctor'S Statement: Patient's Personal DetailsDocument3 pagesMedical Claim - Doctor'S Statement: Patient's Personal DetailsWeng Meng VISTANo ratings yet
- Bajaj Allianz Cashless Request FormDocument3 pagesBajaj Allianz Cashless Request FormM/s MicrotechNo ratings yet
- Easy Health Claim FormDocument4 pagesEasy Health Claim FormQwerty TNo ratings yet
- Easy Health Claim FormDocument4 pagesEasy Health Claim FormAnkithNo ratings yet
- CMRF Form English - FinalDocument3 pagesCMRF Form English - Finalgudepukumar280No ratings yet
- Reliance Health Insurance Pre Authorisation FormDocument4 pagesReliance Health Insurance Pre Authorisation FormM/s MicrotechNo ratings yet
- Put Your LOGO & SLOGAN Here: A. Policyholder - Insured DetailsDocument3 pagesPut Your LOGO & SLOGAN Here: A. Policyholder - Insured DetailsTHÍCH XEM XENo ratings yet
- EEA Application Form v11Document9 pagesEEA Application Form v11Sean SandersNo ratings yet
- Submit Your Health Insurance ClaimDocument2 pagesSubmit Your Health Insurance ClaimsabaNo ratings yet
- MEDICARE CLAIM FORMDocument2 pagesMEDICARE CLAIM FORMtagashiiNo ratings yet
- Reg 2-Primary Care Claim Form-31 Oct 2008Document2 pagesReg 2-Primary Care Claim Form-31 Oct 2008Pradeep KhubchandaniNo ratings yet
- How To Increase The Longevity of AGL Assets PDFDocument36 pagesHow To Increase The Longevity of AGL Assets PDFywa00No ratings yet
- PCC 0500Document4 pagesPCC 0500ywa00No ratings yet
- Chapter 12 Underground Electrical SystemsDocument21 pagesChapter 12 Underground Electrical Systemsywa00No ratings yet
- 150 5340 30g PDFDocument308 pages150 5340 30g PDFLincoln RibeiroNo ratings yet
- Hosts UmbrellaDocument1 pageHosts UmbrellaFabsor SoralNo ratings yet
- Agriculture Calender Page enDocument1 pageAgriculture Calender Page enywa00No ratings yet
- Ac 150-5340-30JDocument396 pagesAc 150-5340-30JHamilton RomeroNo ratings yet
- L-108 Underground Power Cable 609765 7 PDFDocument17 pagesL-108 Underground Power Cable 609765 7 PDFywa00No ratings yet
- OutdoorDocument2 pagesOutdoorywa00No ratings yet
- 2008 GMC Acadia GetknowDocument24 pages2008 GMC Acadia Getknowywa00100% (1)
- AVK Butterfly ValveDocument2 pagesAVK Butterfly Valveywa00No ratings yet
- The Wave - Muscat Main Brochure 2010Document21 pagesThe Wave - Muscat Main Brochure 2010ywa00No ratings yet
- Inter Global Claim Form 2010Document4 pagesInter Global Claim Form 2010ywa00No ratings yet
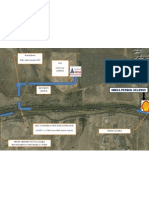
- Amana Site Location MapDocument1 pageAmana Site Location Mapywa00No ratings yet
- Project The Ant Ranch Ponzi Scheme JDDocument7 pagesProject The Ant Ranch Ponzi Scheme JDmorraz360No ratings yet
- Make a Battery Level Indicator using LM339 ICDocument13 pagesMake a Battery Level Indicator using LM339 ICnelson100% (1)
- E-TON - Vector ST 250Document87 pagesE-TON - Vector ST 250mariusgrosyNo ratings yet
- 50TS Operators Manual 1551000 Rev CDocument184 pages50TS Operators Manual 1551000 Rev CraymondNo ratings yet
- Cars Should Be BannedDocument3 pagesCars Should Be BannedIrwanNo ratings yet
- Janapriya Journal of Interdisciplinary Studies - Vol - 6Document186 pagesJanapriya Journal of Interdisciplinary Studies - Vol - 6abiskarNo ratings yet
- Erp and Mis Project - Thanks To PsoDocument31 pagesErp and Mis Project - Thanks To PsoAkbar Syed100% (1)
- Diagnostic Information For Database Replay IssuesDocument10 pagesDiagnostic Information For Database Replay IssuesjjuniorlopesNo ratings yet
- Journal Publication FormatDocument37 pagesJournal Publication FormatAbreo Dan Vincent AlmineNo ratings yet
- Code Description DSMCDocument35 pagesCode Description DSMCAnkit BansalNo ratings yet
- CadLink Flyer 369044 937 Rev 00Document2 pagesCadLink Flyer 369044 937 Rev 00ShanaHNo ratings yet
- Introduction To Succession-1Document8 pagesIntroduction To Succession-1amun dinNo ratings yet
- 2CG ELTT2 KS TitanMagazine Anazelle-Shan PromoDocument12 pages2CG ELTT2 KS TitanMagazine Anazelle-Shan PromoJohn SmithNo ratings yet
- SyllabusDocument4 pagesSyllabusapi-105955784No ratings yet
- 1st Exam Practice Scratch (Answer)Document2 pages1st Exam Practice Scratch (Answer)Tang Hing Yiu, SamuelNo ratings yet
- Welding MapDocument5 pagesWelding MapDjuangNo ratings yet
- Logistic Regression to Predict Airline Customer Satisfaction (LRCSDocument20 pagesLogistic Regression to Predict Airline Customer Satisfaction (LRCSJenishNo ratings yet
- Fujitsu Spoljni Multi Inverter Aoyg45lbt8 Za 8 Unutrasnjih Jedinica KatalogDocument4 pagesFujitsu Spoljni Multi Inverter Aoyg45lbt8 Za 8 Unutrasnjih Jedinica KatalogSasa021gNo ratings yet
- 6vortex 20166523361966663Document4 pages6vortex 20166523361966663Mieczysław MichalczewskiNo ratings yet
- DHPL Equipment Updated List Jan-22Document16 pagesDHPL Equipment Updated List Jan-22jairamvhpNo ratings yet
- Comparing Time Series Models to Predict Future COVID-19 CasesDocument31 pagesComparing Time Series Models to Predict Future COVID-19 CasesManoj KumarNo ratings yet
- Oop Assignment # 2 Submitted By: Hashir Khan Roll #: 22f-7465 Date: 3-3-2023Document14 pagesOop Assignment # 2 Submitted By: Hashir Khan Roll #: 22f-7465 Date: 3-3-2023Hashir KhanNo ratings yet
- BAR Digest MenuDocument4 pagesBAR Digest MenuFloila Jane YmasNo ratings yet
- Tyron Butson (Order #37627400)Document74 pagesTyron Butson (Order #37627400)tyron100% (2)
- Emperger's pioneering composite columnsDocument11 pagesEmperger's pioneering composite columnsDishant PrajapatiNo ratings yet
- Dwnload Full International Monetary Financial Economics 1st Edition Daniels Solutions Manual PDFDocument36 pagesDwnload Full International Monetary Financial Economics 1st Edition Daniels Solutions Manual PDFelegiastepauleturc7u100% (16)
- Novirost Sample TeaserDocument2 pagesNovirost Sample TeaserVlatko KotevskiNo ratings yet
- 04 Dasmarinas Vs Reyes GR No 108229Document2 pages04 Dasmarinas Vs Reyes GR No 108229Victoria Melissa Cortejos PulidoNo ratings yet
- Binaural Recording Technology: A Historical Review and Possible Future DevelopmentsDocument22 pagesBinaural Recording Technology: A Historical Review and Possible Future DevelopmentsNery BorgesNo ratings yet
- Elaspeed Cold Shrink Splices 2010Document3 pagesElaspeed Cold Shrink Splices 2010moisesramosNo ratings yet