You might also like
- Soap NoteDocument2 pagesSoap Notetopopirate100% (4)
- Brain Sheet - Nursing Brain Sheet ExampleDocument1 pageBrain Sheet - Nursing Brain Sheet ExampleShari KvidahlNo ratings yet
- SOAP TemplateDocument3 pagesSOAP Templateazhar100% (1)
- CARAS SCUTSHEET 2nd EditDocument2 pagesCARAS SCUTSHEET 2nd EditFrances Katrina Siruno100% (1)
- H&PEDocument2 pagesH&PEDanielleNo ratings yet
- Hospital Follow Up Progress Note MedicalTemplateDocument1 pageHospital Follow Up Progress Note MedicalTemplatee-MedTools100% (18)
- Hyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Comprehensive H&PDocument2 pagesComprehensive H&PjwwisnerNo ratings yet
- The Nurse Practitioner in UrologyFrom EverandThe Nurse Practitioner in UrologyMichelle LajinessNo ratings yet
- New Assessment Form 2Document5 pagesNew Assessment Form 2api-3739910100% (2)
- History and Physical Examination Checklist PDFDocument10 pagesHistory and Physical Examination Checklist PDFgietsche_gelNo ratings yet
- Brainsheet f04Document2 pagesBrainsheet f04mrsfelic08No ratings yet
- Soap Note Template 03Document5 pagesSoap Note Template 03Razan HaimounyNo ratings yet
- Student Worksheet2023 PDFDocument2 pagesStudent Worksheet2023 PDFjj100% (1)
- Patient History and Presentation SkillsDocument4 pagesPatient History and Presentation Skillsbnarnold100% (2)
- Primary Care FollowupDocument1 pagePrimary Care Followupe-MedTools100% (6)
- New Icu SheetDocument3 pagesNew Icu SheetJan MarcusNo ratings yet
- Clinical KardexDocument2 pagesClinical KardexJackie Frey100% (2)
- CC: Demo: Hpi: Allergies: Pertinent ROS: Vitals:: LabsDocument4 pagesCC: Demo: Hpi: Allergies: Pertinent ROS: Vitals:: Labsagrawa03No ratings yet
- Soap TemplateDocument3 pagesSoap TemplaterohitNo ratings yet
- Pneumonia Cheat Sheet: by ViaDocument3 pagesPneumonia Cheat Sheet: by ViaGayle MarieNo ratings yet
- 2019 Pediatric Clinical Note Template-2Document6 pages2019 Pediatric Clinical Note Template-2samNo ratings yet
- Nursing SheetDocument1 pageNursing Sheetseaturtles505100% (1)
- 3 SOAP Presentation Template 5.19.16 PDFDocument1 page3 SOAP Presentation Template 5.19.16 PDFnems92No ratings yet
- Clinical Organization Sheet NursingDocument1 pageClinical Organization Sheet NursingSarah S100% (1)
- Physical Exam ChecklistDocument1 pagePhysical Exam ChecklistLaura Hernandez100% (5)
- Health HistoryDocument19 pagesHealth HistoryAngelene Caliva100% (1)
- H&P OutlineDocument5 pagesH&P Outlineginadaislu100% (1)
- History & Physical Diagnostic#Document106 pagesHistory & Physical Diagnostic#Olsa Alshapira100% (1)
- Care Plan Handbook TemplateDocument34 pagesCare Plan Handbook TemplateBreanna Hopkins100% (1)
- The Intern Pocket Card Surviving GraysDocument2 pagesThe Intern Pocket Card Surviving GraysKathleen Grace ManiagoNo ratings yet
- Write Up TutorialDocument22 pagesWrite Up Tutorialballer0417100% (1)
- HPI For History and Physical ExamDocument2 pagesHPI For History and Physical Examv-santNo ratings yet
- Hypertension Follow Up EvaluationDocument1 pageHypertension Follow Up Evaluatione-MedTools100% (3)
- Isolation:: Orders To Flush Central/hep Loc line/PICCDocument1 pageIsolation:: Orders To Flush Central/hep Loc line/PICCmmaturNo ratings yet
- Charting GuidelinesDocument4 pagesCharting Guidelinesgrad_nurse_2015No ratings yet
- Interview Pa Tool.Document5 pagesInterview Pa Tool.Raisah Bint AbdullahNo ratings yet
- MS3 Survival GuideDocument50 pagesMS3 Survival Guideprahul2588No ratings yet
- Pediatric Assessment: General ImpressionDocument2 pagesPediatric Assessment: General ImpressionAghnia Nafila100% (1)
- Assessment CardsDocument3 pagesAssessment CardsLindsay Couillard100% (3)
- WARDWORK TemplateDocument9 pagesWARDWORK TemplateColeen NeyraNo ratings yet
- General History and Physical Examination FormDocument2 pagesGeneral History and Physical Examination FormQueen Hera100% (1)
- Megs History PhysicalDocument1 pageMegs History Physicalrmelendez001No ratings yet
- Case PresentationDocument30 pagesCase PresentationAmira HelayelNo ratings yet
- BrainSheet 2patient v3Document1 pageBrainSheet 2patient v3Shelly BassNo ratings yet
- Gram Positive Cocci (GPC) Gram Neg (Rods GNR) Anaerobes Atypicals Classification AntibioticDocument2 pagesGram Positive Cocci (GPC) Gram Neg (Rods GNR) Anaerobes Atypicals Classification AntibioticRami RaedNo ratings yet
- Medicine1 Grand PE ScriptDocument10 pagesMedicine1 Grand PE ScriptCarmeline Santi BeronillaNo ratings yet
- ICU Report SheetDocument2 pagesICU Report SheetShelby Sheppard100% (1)
- Uncle Rays OB-GYN Reference 09-10Document153 pagesUncle Rays OB-GYN Reference 09-10goyobaNo ratings yet
- Clinical Examinations Crib Sheet v7Document36 pagesClinical Examinations Crib Sheet v7aparish10100% (1)
- GSS ScutsheetDocument2 pagesGSS ScutsheetAndy FischerNo ratings yet
- Word AssociationDocument27 pagesWord AssociationMilan Kolovrat100% (1)
- Audit FormsDocument4 pagesAudit Formsapi-349641525No ratings yet
- Suggested Word List For DocumentationDocument1 pageSuggested Word List For Documentationjkbills100% (6)
- FNP Prelims Reviewer PDFDocument29 pagesFNP Prelims Reviewer PDFJOSHUA TORRICERNo ratings yet
- Common Signs and SymptomsDocument36 pagesCommon Signs and SymptomsJamil AimanNo ratings yet
- HaruyamaDocument10 pagesHaruyamabarros6No ratings yet
- Abdomen IntroductionDocument32 pagesAbdomen Introductionpixiemedic100% (1)
- Maya RigDocument329 pagesMaya Rigskynet24100% (2)
- N222 Lecture Notes Sp13Document198 pagesN222 Lecture Notes Sp13Jacinth Florido FedelinNo ratings yet
- CHEK Scientific Core Conditioning PDFDocument246 pagesCHEK Scientific Core Conditioning PDFLuz Divina Casalins100% (14)
- Shape Up With Caroline Sandry's Pilates WorkoutDocument4 pagesShape Up With Caroline Sandry's Pilates WorkoutCaroline Sandry100% (3)
- Shoulder Rehab Book v4 Book PDFDocument178 pagesShoulder Rehab Book v4 Book PDFas as100% (1)
- Normal Labour AND Delivery: Prof DR Mohd Azhar MNDocument90 pagesNormal Labour AND Delivery: Prof DR Mohd Azhar MNLiezel CauilanNo ratings yet
- Genital Prolapse and HomoeopathyDocument69 pagesGenital Prolapse and HomoeopathyAnmol AgrawalNo ratings yet
- The Book of KnowledgeDocument12 pagesThe Book of KnowledgeToh Jing Hua100% (2)
- Anatomy of The PelvisDocument149 pagesAnatomy of The PelvisObongsamuel IdiongNo ratings yet
- Tinjauan Pustaka Persalinan NormalDocument31 pagesTinjauan Pustaka Persalinan NormalNurul Fathia Shafira AmiantiNo ratings yet
- Rehab U LowerbodymobilityDocument11 pagesRehab U Lowerbodymobilityjody.eth.gonzalesNo ratings yet
- What Are The Parts of The Male External Sexual Anatomy?Document3 pagesWhat Are The Parts of The Male External Sexual Anatomy?bla blaNo ratings yet
- Lab 4 - The Skeletal SystemDocument38 pagesLab 4 - The Skeletal SystemNatalie PembertonNo ratings yet
- Tugas Koding: Merlindi HestiaraDocument9 pagesTugas Koding: Merlindi HestiaraShafiaNo ratings yet
- AP MusclesDocument14 pagesAP MusclesAlexandra NadinneNo ratings yet
- Mcgill 2010Document15 pagesMcgill 2010Júnior Alvacir CamargoNo ratings yet
- Zona Neutra Wallden, 2009Document12 pagesZona Neutra Wallden, 2009anon_861143750No ratings yet
- Casts. Braces. TractionDocument3 pagesCasts. Braces. TractionClancy Anne Garcia Naval100% (1)
- Coding ZupkoDocument8 pagesCoding Zupkoashwanirana09No ratings yet
- Antenatal ExercisesDocument8 pagesAntenatal ExercisesedrinsneNo ratings yet
- 3B Scientific CompleteDocument154 pages3B Scientific CompleteMohammad Izham Ismail100% (1)
- Cardinal Movements of LaborDocument2 pagesCardinal Movements of LaborAimhigh_PPM100% (1)
- Imaging in Genitourinary SystemDocument36 pagesImaging in Genitourinary SystemAlkaustariyah LubisNo ratings yet
- Strategic Intervention MaterialDocument9 pagesStrategic Intervention MaterialHana Karudi100% (1)
- Introduction To The NETA Pilates Home Study Certificate Course (PDFDrive)Document178 pagesIntroduction To The NETA Pilates Home Study Certificate Course (PDFDrive)Azaan NavidNo ratings yet
- Chapter 2 f5Document103 pagesChapter 2 f5Jo YeeNo ratings yet
- Wo Jahn 2019Document10 pagesWo Jahn 2019Fauzan KurniawanNo ratings yet
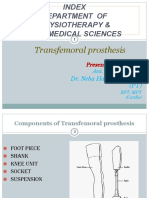
- TRANSFEMORAL - PPT 1Document64 pagesTRANSFEMORAL - PPT 1Farheen KhanNo ratings yet