You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pharmacology Alphabet AllDocument4 pagesPharmacology Alphabet Allsflower85No ratings yet
- Bacterial Meningitis PDFDocument18 pagesBacterial Meningitis PDFZulaicha MumarridzohNo ratings yet
- Psiquiatría - Delirium y DemenciaDocument11 pagesPsiquiatría - Delirium y DemenciaPediatrics - Pediatric SurgeryNo ratings yet
- Croup, Crup, LaringotraqueobronquitisDocument6 pagesCroup, Crup, LaringotraqueobronquitisPediatrics - Pediatric SurgeryNo ratings yet
- Urología - EpididimitisDocument8 pagesUrología - EpididimitisPediatrics - Pediatric SurgeryNo ratings yet
- Gestational Trophoblastic Disease - Enfermedad Trofoblastica GestacionalDocument9 pagesGestational Trophoblastic Disease - Enfermedad Trofoblastica GestacionalPediatrics - Pediatric SurgeryNo ratings yet
- Crisis Hipertensivas - Hypertensive CrisesDocument13 pagesCrisis Hipertensivas - Hypertensive CrisesPediatrics - Pediatric SurgeryNo ratings yet
- Insuficiencia Renal Aguda (The Patient With Acute Kidney Injury)Document26 pagesInsuficiencia Renal Aguda (The Patient With Acute Kidney Injury)Pediatrics - Pediatric SurgeryNo ratings yet
- Rinitis AlérgicaDocument8 pagesRinitis AlérgicaPediatrics - Pediatric SurgeryNo ratings yet
- Lower Urinary Tract Symptoms - The Management of Lower Urinary Tract Symptoms in MenDocument34 pagesLower Urinary Tract Symptoms - The Management of Lower Urinary Tract Symptoms in MenPediatrics - Pediatric Surgery100% (1)
- Hipotiroidismo - HypothyroidismDocument21 pagesHipotiroidismo - HypothyroidismPediatrics - Pediatric SurgeryNo ratings yet
- Nefrología - Desequilibrio Ácido-BaseDocument41 pagesNefrología - Desequilibrio Ácido-BasePediatrics - Pediatric SurgeryNo ratings yet
- Benign Prostatic HyperplasiaDocument15 pagesBenign Prostatic HyperplasiaPediatrics - Pediatric SurgeryNo ratings yet
- Endocriniología - Hyperglicemic Crisis in Adult Patients With DiabetesDocument10 pagesEndocriniología - Hyperglicemic Crisis in Adult Patients With DiabetesPediatrics - Pediatric SurgeryNo ratings yet
- Historia de La Medicina - Sydney Ringer & Alexis HartmannDocument8 pagesHistoria de La Medicina - Sydney Ringer & Alexis HartmannPediatrics - Pediatric SurgeryNo ratings yet
- Pediatría - Desarrollo y CrecimientoDocument19 pagesPediatría - Desarrollo y CrecimientoPediatrics - Pediatric SurgeryNo ratings yet
- Grafik CDCDocument10 pagesGrafik CDCArief Budi LesmanaNo ratings yet
- Neurología - Foster Kennedy SyndromeDocument4 pagesNeurología - Foster Kennedy SyndromePediatrics - Pediatric SurgeryNo ratings yet
- Pediatría - Hypertension in Children and AdolescentsDocument11 pagesPediatría - Hypertension in Children and AdolescentsPediatrics - Pediatric Surgery100% (1)
- Endocrinología - Polycystic Ovary SyndromeDocument14 pagesEndocrinología - Polycystic Ovary SyndromePediatrics - Pediatric SurgeryNo ratings yet
- Pediatría - Leucemias en PediatríaDocument24 pagesPediatría - Leucemias en PediatríaPediatrics - Pediatric SurgeryNo ratings yet
- Pediatría - HipotiroidismoDocument7 pagesPediatría - HipotiroidismoPediatrics - Pediatric SurgeryNo ratings yet
- Pediatría - Anemia in ChildrenDocument8 pagesPediatría - Anemia in ChildrenPediatrics - Pediatric SurgeryNo ratings yet
- Self-Assessment Questions Chapter 8 The Urinary SystemDocument10 pagesSelf-Assessment Questions Chapter 8 The Urinary Systemsanam shahzadi100% (1)
- NCLEX Review Cardiovascular QuizDocument17 pagesNCLEX Review Cardiovascular Quizdany tesemaNo ratings yet
- Blood Pressure RegulationDocument51 pagesBlood Pressure RegulationBangkit Benedikta Hutcherson100% (1)
- CP (Sub-Grp)Document79 pagesCP (Sub-Grp)Pamela laquindanumNo ratings yet
- Adrenal HormonesDocument62 pagesAdrenal HormonesM.PRASAD NAIDUNo ratings yet
- Saltwater Power: Samal National High SchoolDocument47 pagesSaltwater Power: Samal National High SchoolKhloe EppohsNo ratings yet
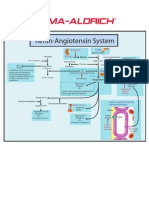
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- ARBs (Angiotensin II Receptor Blockers) NCLEXDocument15 pagesARBs (Angiotensin II Receptor Blockers) NCLEXSameerQadumi100% (1)
- Ch-13 Drugs Used in Heart FailureDocument49 pagesCh-13 Drugs Used in Heart FailureShabrin SadikhNo ratings yet
- Neurologic Manifestations of Major Electrolyte AbnormalitiesDocument9 pagesNeurologic Manifestations of Major Electrolyte AbnormalitiesMartha OktaviaNo ratings yet
- Body Fluids-1: Fluid Compartments of The Body Fluid and Electrolyte CompositionDocument33 pagesBody Fluids-1: Fluid Compartments of The Body Fluid and Electrolyte CompositionMan LingNo ratings yet
- What Is Hyperaldosteronism?Document7 pagesWhat Is Hyperaldosteronism?sajad abasNo ratings yet
- Anatomy and Physiology of Farm Animals GuideDocument51 pagesAnatomy and Physiology of Farm Animals Guidealexenneth canilaNo ratings yet
- Azelnidipine Effects on Renin and AldosteroneDocument7 pagesAzelnidipine Effects on Renin and Aldosteronergp1089No ratings yet
- Return To The Medical Biochemistry PageDocument8 pagesReturn To The Medical Biochemistry Pagevibhav82No ratings yet
- Endocrine Anatomy 4Document16 pagesEndocrine Anatomy 4Snehal JayaramNo ratings yet
- Disorders of Sodium and Potassium MetabolismDocument18 pagesDisorders of Sodium and Potassium MetabolismTukuWoNo ratings yet
- Mabes Fluid and ElectrolytesDocument9 pagesMabes Fluid and ElectrolytesMabesNo ratings yet
- Regulating Renal Blood Flow and Glomerular FiltrationDocument41 pagesRegulating Renal Blood Flow and Glomerular FiltrationAfk SystemNo ratings yet
- English Sistem EndocrineDocument9 pagesEnglish Sistem EndocrineNurlaili YaniNo ratings yet
- The Renin-Angiotensin Aldosterone System: Pathophysiological Role and Pharmacologic InhibitionDocument12 pagesThe Renin-Angiotensin Aldosterone System: Pathophysiological Role and Pharmacologic Inhibitionfatimah hasibuanNo ratings yet
- Electrolyte and Acid Base DisordersDocument46 pagesElectrolyte and Acid Base DisordersMia ValdesNo ratings yet
- Blood Vessels and Respiratory Practice QuestionsDocument15 pagesBlood Vessels and Respiratory Practice QuestionsRACHEL VERA RODRIGUEZNo ratings yet
- Ascites Causes Diagnosis and TreatmentDocument24 pagesAscites Causes Diagnosis and TreatmentrifkaNo ratings yet
- Endocrinology InterpretationDocument382 pagesEndocrinology InterpretationHernanda Adi Purwangga100% (7)
- Renal Embryology: Jason Ryan, MD, MPHDocument731 pagesRenal Embryology: Jason Ryan, MD, MPHFateh BoulounisNo ratings yet
- Aquatic Physics: Relative DensityDocument18 pagesAquatic Physics: Relative DensitymilananandNo ratings yet
- Hormonal Control of Metabolism During ExerciseDocument32 pagesHormonal Control of Metabolism During ExerciseamirNo ratings yet
- Chapter 3 Fluids and Electrolytes - Acid-Base BalanceDocument8 pagesChapter 3 Fluids and Electrolytes - Acid-Base BalanceDiony CruzNo ratings yet