You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Heart Valve Disease: State of the ArtFrom EverandHeart Valve Disease: State of the ArtJose ZamoranoNo ratings yet
- Near Drowning Emedicine SpecialtiesDocument9 pagesNear Drowning Emedicine SpecialtiesIntan Eklesiana NapitupuluNo ratings yet
- Pathophysiology DrowningDocument13 pagesPathophysiology DrowningIndah HaneNo ratings yet
- DrowningDocument14 pagesDrowningkrisnandarNo ratings yet
- DrowningDocument7 pagesDrowningAidaDenisse Negrete DurazoNo ratings yet
- 11 - Shock - Current Diagnosis and Treatment Emergency MedicineDocument18 pages11 - Shock - Current Diagnosis and Treatment Emergency MedicineRon KNo ratings yet
- Choque en Urgencias 2018Document14 pagesChoque en Urgencias 2018Aura María Salazar SolarteNo ratings yet
- Travel Medicine Drowning 2015Document11 pagesTravel Medicine Drowning 2015Nym Angga SantosaNo ratings yet
- Final File 5b3f0331f0f340.99334869Document4 pagesFinal File 5b3f0331f0f340.99334869Amirullah AbdiNo ratings yet
- Paediatric Respiratory Reviews: F. Healy, B.D. Hanna, R. ZinmanDocument6 pagesPaediatric Respiratory Reviews: F. Healy, B.D. Hanna, R. ZinmanfadmayulianiNo ratings yet
- Shock Management in Children: Nora SoviraDocument6 pagesShock Management in Children: Nora Soviraminerva-larasatiNo ratings yet
- Decompression IllnessDocument12 pagesDecompression Illnesstonylee24No ratings yet
- Shock - Critical Care Medicine - MSD Manual Professional EditionDocument8 pagesShock - Critical Care Medicine - MSD Manual Professional EditionSughosh MitraNo ratings yet
- Circulatory Shock in Children:: An OverviewDocument10 pagesCirculatory Shock in Children:: An Overviewsugarp_3No ratings yet
- Hypoxia and Stroke: "2% in Younger Adults, But in Healthy Older PeopleDocument3 pagesHypoxia and Stroke: "2% in Younger Adults, But in Healthy Older PeopleJerahmeel Sombilon GenillaNo ratings yet
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- Hypovolemic Shock - A Review: Drug Invention Today July 2018Document5 pagesHypovolemic Shock - A Review: Drug Invention Today July 2018AndreasNo ratings yet
- Shock 20231122 213304 0000Document32 pagesShock 20231122 213304 0000Mikella E. PAGNAMITANNo ratings yet
- Evidence Based Reading - FormatDocument2 pagesEvidence Based Reading - FormatMarvie TorralbaNo ratings yet
- Complications of Extremeitiy TraumaDocument11 pagesComplications of Extremeitiy TraumaGilang Kurnia HirawatiNo ratings yet
- Traumatic AsphyxiaDocument15 pagesTraumatic AsphyxiaAnil AggrawalNo ratings yet
- Evidence Based Reading FormatDocument2 pagesEvidence Based Reading FormatMarvie TorralbaNo ratings yet
- Hemorrhagic ShockDocument11 pagesHemorrhagic ShockmuamervukNo ratings yet
- Critical Care Management of Acute Stroke - ZazuliaDocument15 pagesCritical Care Management of Acute Stroke - ZazuliaIndah ManafNo ratings yet
- Shock and Blood TransfusionDocument41 pagesShock and Blood TransfusionpalNo ratings yet
- Disorders of The PulpDocument7 pagesDisorders of The Pulpابو الجودNo ratings yet
- Intensive MedicineDocument17 pagesIntensive MedicinehasebeNo ratings yet
- Hypovolemic ShockDocument10 pagesHypovolemic ShockUsran Ali BubinNo ratings yet
- Hanhan 2001Document12 pagesHanhan 2001ATIKAH NUR HAFIZHAHNo ratings yet
- Drowning: David Szpilman, James P. Orlowski, and Joost BierensDocument8 pagesDrowning: David Szpilman, James P. Orlowski, and Joost BierensIhsan M NauvalNo ratings yet
- Hypertensive Vascular DiseaseDocument5 pagesHypertensive Vascular DiseaseGenoMacaraanNo ratings yet
- DrowningDocument27 pagesDrowningDwi Anggraeni100% (1)
- Referensi 7 PDFDocument5 pagesReferensi 7 PDFirfhanahusaNo ratings yet
- Lecture 10Document13 pagesLecture 10Grafu Andreea AlexandraNo ratings yet
- The Management of Near DrowningDocument8 pagesThe Management of Near DrowningneddiantiseptikaNo ratings yet
- Critical Care in The Emergency Department: Shock and Circulatory SupportDocument10 pagesCritical Care in The Emergency Department: Shock and Circulatory SupportKhaled AbdoNo ratings yet
- Distributive ShockDocument26 pagesDistributive ShockYorim Sora PasilaNo ratings yet
- Hypovolemic Shock 09Document58 pagesHypovolemic Shock 09Joanne Bernadette Aguilar100% (2)
- Hypovolemic Shock in Patient With Burn TraumaDocument11 pagesHypovolemic Shock in Patient With Burn TraumaSundhias Larashati100% (1)
- Trauma Lethal TriadDocument10 pagesTrauma Lethal TriadChristian Kuon-YengNo ratings yet
- Acute Respiratory Distress SyndromeDocument17 pagesAcute Respiratory Distress SyndromeSanjeet SahNo ratings yet
- Hypovolemic Shock in ChildrenDocument5 pagesHypovolemic Shock in ChildrenSussy ListiarsasihNo ratings yet
- Sachdeva 1999 Near DrowningDocument16 pagesSachdeva 1999 Near Drowninghartanto_budi6222No ratings yet
- Drowning - WFSADocument6 pagesDrowning - WFSAcorinna.ongaigui.gsbmNo ratings yet
- Wardclass-Venous Air EmbolismDocument17 pagesWardclass-Venous Air EmbolismDan Dan Soi TNo ratings yet
- Physiology of Drowning PDFDocument63 pagesPhysiology of Drowning PDFPeter PhelpsNo ratings yet
- Background: EmbryologyDocument25 pagesBackground: EmbryologydonisaputraNo ratings yet
- DrowningDocument28 pagesDrowningjparker35045No ratings yet
- AKI (Pre Renal - Intra Renal - Post Renal)Document14 pagesAKI (Pre Renal - Intra Renal - Post Renal)Ashraf QotmoshNo ratings yet
- Definisi Kak DiniDocument2 pagesDefinisi Kak DiniAulia Achmad Yudha PratamaNo ratings yet
- ShockDocument9 pagesShockapocruNo ratings yet
- Shock - Critical Care Medicine - MSD Manual Professional EditionDocument11 pagesShock - Critical Care Medicine - MSD Manual Professional Editionazaria zhafirahNo ratings yet
- Case ReportDocument49 pagesCase ReportMageswari SelvarajooNo ratings yet
- Syncope (Medicine)Document7 pagesSyncope (Medicine)Wira SentanuNo ratings yet
- Hemorrhagic Shock - StatPearls - NCBI BookshelfDocument8 pagesHemorrhagic Shock - StatPearls - NCBI BookshelfRizqan Fahlevvi AkbarNo ratings yet
- Muiz Seminar ProjectDocument28 pagesMuiz Seminar ProjectPrecious AdeshinaNo ratings yet
- Practice of NCC Hypoxic-Ischemic Encephalopathy in AdultsDocument24 pagesPractice of NCC Hypoxic-Ischemic Encephalopathy in AdultsAna Rica Santiago Navarra-CruzNo ratings yet
- AN 623 - Adult Nursing Skills Underpinning Complex Care CW1Document15 pagesAN 623 - Adult Nursing Skills Underpinning Complex Care CW1Gareth McKnight100% (2)
- ShockDocument11 pagesShockNatalia WiryantoNo ratings yet
- Life in Sparta PDFDocument2 pagesLife in Sparta PDFGabriel BispoNo ratings yet
- Final Paper: Patriot ActDocument12 pagesFinal Paper: Patriot Actblaznspadz100% (1)
- D.E. 17-35 Def. JT Mot. Sanctions, 3.11.19Document37 pagesD.E. 17-35 Def. JT Mot. Sanctions, 3.11.19larry-612445No ratings yet
- Jewish Daily Life in Roman Palestine, 2010, 4, OCRDocument8 pagesJewish Daily Life in Roman Palestine, 2010, 4, OCRJoaquín Porras Ordieres100% (1)
- Application For ProbationDocument3 pagesApplication For Probationlobayto lang-ayNo ratings yet
- Torts BDocument15 pagesTorts Byin-pasiya nabiaNo ratings yet
- NEAT Cell State-Wise Distribution of No. of Free SeatsDocument1 pageNEAT Cell State-Wise Distribution of No. of Free SeatsBE19FO3FO66 DnyaneshwarNo ratings yet
- Course Outline in Administrative Law: Every Wednesday, 6:00 PM - 9:00 PM)Document7 pagesCourse Outline in Administrative Law: Every Wednesday, 6:00 PM - 9:00 PM)asfaedNo ratings yet
- Abacus Real Estate Development v. Manila Banking Corporation, G.R. No. 162270, April 6, 2005Document2 pagesAbacus Real Estate Development v. Manila Banking Corporation, G.R. No. 162270, April 6, 2005Metsuyo BariteNo ratings yet
- Electoral College For SindhDocument4 pagesElectoral College For SindhPTI OfficialNo ratings yet
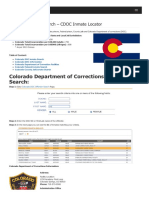
- Colorado Inmate Search Department of Corrections LookupDocument9 pagesColorado Inmate Search Department of Corrections LookupinmatesearchinfoNo ratings yet
- Salary Standardization Rates For Philippine Government EmployeesDocument10 pagesSalary Standardization Rates For Philippine Government Employeesjoebell.gpNo ratings yet
- Causes of Separation of East PakistanDocument5 pagesCauses of Separation of East Pakistantanvir91% (35)
- Hatziefstathiou, Original Media Et Al vs. Montco Dao Oor Docket AP 2021-0009Document56 pagesHatziefstathiou, Original Media Et Al vs. Montco Dao Oor Docket AP 2021-0009Your ContentNo ratings yet
- Since 1894 Painful LinesDocument1 pageSince 1894 Painful Lineswocavi260650% (2)
- Nombrado v. Hernandez (Full Case)Document4 pagesNombrado v. Hernandez (Full Case)Katherine EvangelistaNo ratings yet
- Cloe Ii Eu Institutions Octombrie 2022Document62 pagesCloe Ii Eu Institutions Octombrie 2022clementmihaiNo ratings yet
- Rizal's Social Origins and Historical Context: Overview of Module 2Document14 pagesRizal's Social Origins and Historical Context: Overview of Module 2NeilLaurrenceDimalNo ratings yet
- DT Hot TipsDocument12 pagesDT Hot TipsChaNo ratings yet
- Syllabus: Cambridge O Level Pakistan Studies 2059Document38 pagesSyllabus: Cambridge O Level Pakistan Studies 2059Osama GillNo ratings yet
- Law of AgencyDocument12 pagesLaw of AgencyMuna Farhana100% (7)
- JawsDocument2 pagesJawsted stapletonNo ratings yet
- Unit IV (A) - Arbitration: Aaditya Vikram SharmaDocument17 pagesUnit IV (A) - Arbitration: Aaditya Vikram SharmaNiraj PandeyNo ratings yet
- Hochstrasser (Inspector of Taxes) V MayesDocument3 pagesHochstrasser (Inspector of Taxes) V MayesRafayel MarufNo ratings yet
- Town of Midland Bylaw 98-42Document2 pagesTown of Midland Bylaw 98-42Midland_MirrorNo ratings yet
- Romance of The Rose (Critical Analysis)Document3 pagesRomance of The Rose (Critical Analysis)Mark MerrillNo ratings yet
- Deed of Absolute Sale - Digol and Discipulo - 041818Document5 pagesDeed of Absolute Sale - Digol and Discipulo - 041818Geoffrey Gitamondoc CagakitNo ratings yet
- Saint NicholasDocument1 pageSaint NicholassqueekymccleanNo ratings yet
- Distress For Rent ActDocument20 pagesDistress For Rent Actjaffar s mNo ratings yet
- 15 Sonal PatilDocument7 pages15 Sonal PatilAnonymous CwJeBCAXpNo ratings yet