You might also like
- Nursing Care Plan Cholecystectomy Gall Bladder RemovalDocument2 pagesNursing Care Plan Cholecystectomy Gall Bladder Removalderic100% (16)
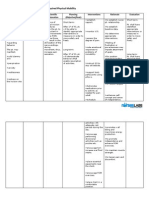
- Impaired Physical Mobility CholecystectomyDocument2 pagesImpaired Physical Mobility CholecystectomyPrincess Danica Purcia100% (1)
- Cholecystectomy Nursing Care Plan: Post-Operative Acute PainDocument2 pagesCholecystectomy Nursing Care Plan: Post-Operative Acute PainCherald Paul C AsuncionNo ratings yet
- Activity Intolerance CholecystectomyDocument2 pagesActivity Intolerance CholecystectomyPrincess Danica Purcia100% (3)
- CHolelytiasisDocument1 pageCHolelytiasisPrincess Danica PurciaNo ratings yet
- Nursing Care Plan CholelithiasisDocument2 pagesNursing Care Plan Cholelithiasisderic97% (36)
- Essential Knot Tying Guide for Rope, String & MoreDocument2 pagesEssential Knot Tying Guide for Rope, String & MorePrincess Danica PurciaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Scio Four Gas Module Family: Reliable and Flexible Gas AnalysisDocument2 pagesScio Four Gas Module Family: Reliable and Flexible Gas AnalysisNasr Eldin AlyNo ratings yet
- Influence of Cavity LiningDocument7 pagesInfluence of Cavity Liningpatel keralNo ratings yet
- Blood Pressure Log 30Document2 pagesBlood Pressure Log 30Yousab KaldasNo ratings yet
- Evaluation of scales in immune-mediated polyneuropathiesDocument222 pagesEvaluation of scales in immune-mediated polyneuropathiesAngelo MalerbaNo ratings yet
- MGR Medical University Medal WinnersDocument17 pagesMGR Medical University Medal WinnersElavarasanNo ratings yet
- Sound Transduction EarDocument7 pagesSound Transduction Earhsc5013100% (1)
- Grievously: News Item 9: EARTHQUAKE 2Document2 pagesGrievously: News Item 9: EARTHQUAKE 2roxana_boraNo ratings yet
- JK SCIENCE: Verrucous Carcinoma of the Mobile TongueDocument3 pagesJK SCIENCE: Verrucous Carcinoma of the Mobile TonguedarsunaddictedNo ratings yet
- Inspiring With Cystic FibrosisDocument2 pagesInspiring With Cystic FibrosisBeverlyHillsWeeklyNo ratings yet
- Raising Dengue Awareness in the PhilippinesDocument4 pagesRaising Dengue Awareness in the PhilippinesAlyssa Hazza Membrano MayonadoNo ratings yet
- Rope NegotiationDocument4 pagesRope NegotiationTH x TH100% (1)
- Jurnal Hubungan Kecemasan Dengan Kepuasan KeluargaDocument10 pagesJurnal Hubungan Kecemasan Dengan Kepuasan KeluargaSri permata DewiNo ratings yet
- The LungsDocument6 pagesThe LungsnandaNo ratings yet
- Return Demonstration: Urinary Catheterization Perineal CareDocument3 pagesReturn Demonstration: Urinary Catheterization Perineal CareDebbie beeNo ratings yet
- Misoprostole in ObstetricsDocument11 pagesMisoprostole in ObstetricsDr-Saja O. DmourNo ratings yet
- Gambaran CT SCAN: (Kasus: Edh, SDH, Ich, Sah, Infark Cerebri, IvhDocument44 pagesGambaran CT SCAN: (Kasus: Edh, SDH, Ich, Sah, Infark Cerebri, Ivhfahmi rosyadiNo ratings yet
- Emergency Preparedness Concepts Test BankDocument13 pagesEmergency Preparedness Concepts Test BankTyson Easo JonesNo ratings yet
- Obesity Exercise PrescriptionDocument34 pagesObesity Exercise Prescriptionkhushbu88% (8)
- Older Adults Group PlanDocument31 pagesOlder Adults Group Planapi-316614503No ratings yet
- Abigail BDocument3 pagesAbigail BbjhilarioNo ratings yet
- Zocor (Simvastatin)Document3 pagesZocor (Simvastatin)E100% (1)
- Diagnostic Imaging Equipment & Consumables Laser PrintersDocument5 pagesDiagnostic Imaging Equipment & Consumables Laser Printersnanu_gomezNo ratings yet
- PTP1 - Reading Test 5Document17 pagesPTP1 - Reading Test 5Anh DucNo ratings yet
- CCMP 2020 Batch Cardiovascular MCQsDocument2 pagesCCMP 2020 Batch Cardiovascular MCQsharshad patelNo ratings yet
- Nursing Care Plan HydrocephalusDocument7 pagesNursing Care Plan HydrocephalusFarnii MarquezNo ratings yet
- Case Study of Mrs. WalkerDocument4 pagesCase Study of Mrs. WalkerPreet ChahalNo ratings yet
- Science 5Document81 pagesScience 5Michael Joseph Santos100% (2)
- The JFK AutopsyDocument6 pagesThe JFK AutopsysithusoemoeNo ratings yet
- v1 High Sensitivity C-Reactive Protein HSCDocument2 pagesv1 High Sensitivity C-Reactive Protein HSCKhendy SugihartoNo ratings yet
- Alabama Board of Medical Examiners Statement On Federal Pill Mill TakedownDocument103 pagesAlabama Board of Medical Examiners Statement On Federal Pill Mill TakedownAshley RemkusNo ratings yet