You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CMM 25-11-466529430584234180428Document288 pagesCMM 25-11-466529430584234180428Radmanovic Uros MrmyNo ratings yet
- P-L-N-Statistik 2011Document104 pagesP-L-N-Statistik 2011Ahmad AfandiNo ratings yet
- GSM BSS Integration For Field Maintenance: ExercisesDocument14 pagesGSM BSS Integration For Field Maintenance: Exercisesswr cluster100% (1)
- YALE (C878) GDP135VX LIFT TRUCK Service Repair Manual PDFDocument20 pagesYALE (C878) GDP135VX LIFT TRUCK Service Repair Manual PDFfjskekdmmemNo ratings yet
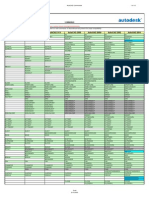
- Autocad R12 Autocad R13 Autocad R14 Autocad 2000 Autocad 2000I Autocad 2002 Autocad 2004Document12 pagesAutocad R12 Autocad R13 Autocad R14 Autocad 2000 Autocad 2000I Autocad 2002 Autocad 2004veteranul13No ratings yet
- System Development Process: The Incremental Commitment ModelDocument20 pagesSystem Development Process: The Incremental Commitment Modeloctopus2011No ratings yet
- Appexchange Publishing GuideDocument29 pagesAppexchange Publishing GuideHeatherNo ratings yet
- Crichton, Michael - NextDocument351 pagesCrichton, Michael - NextrtarakNo ratings yet
- BC-5800 Liquid SystemDocument114 pagesBC-5800 Liquid SystemДмитрийNo ratings yet
- Golden Sun CNC-201R Rotary TableDocument10 pagesGolden Sun CNC-201R Rotary TableGerald100% (2)
- Hydrograph - Analysis - 2 Hydro PDFDocument68 pagesHydrograph - Analysis - 2 Hydro PDFNurul QurratuNo ratings yet
- Automatic Railway Gate Control SystemDocument24 pagesAutomatic Railway Gate Control SystemDIPAK VINAYAK SHIRBHATE100% (12)
- Digital Marketing Course India SyllabusDocument34 pagesDigital Marketing Course India SyllabusAmit KumarNo ratings yet
- Solar Street LightDocument8 pagesSolar Street LightAlizaIbrahim0% (2)
- Greenhouse Project Interim ReportDocument26 pagesGreenhouse Project Interim ReportMuneek ShahNo ratings yet
- HabaCHIAN Slat Conveyor ChainsDocument128 pagesHabaCHIAN Slat Conveyor Chainsjunico76No ratings yet
- Alufusion Eng TrocalDocument226 pagesAlufusion Eng TrocalSid SilviuNo ratings yet
- 9 3 21 Compair Atvt enDocument4 pages9 3 21 Compair Atvt enAcika PeleNo ratings yet
- Six Sigma Green Belt Training Statistical Self Assessment ToolDocument5 pagesSix Sigma Green Belt Training Statistical Self Assessment Toolashutoshsingh2302No ratings yet
- API 580 NotesDocument2 pagesAPI 580 Notesmallesh100% (2)
- Fire Hydrant - WikipediaDocument9 pagesFire Hydrant - WikipediaVaibhav SawantNo ratings yet
- Códigos de Fallas de Problemas Específicos de PEUGEOTDocument8 pagesCódigos de Fallas de Problemas Específicos de PEUGEOTJesus GarciaNo ratings yet
- Light Runner BrochureDocument4 pagesLight Runner Brochureguruprasad19852011No ratings yet
- The Running and Maintenance ofDocument459 pagesThe Running and Maintenance ofantonigor100% (1)
- 2005 TJ BodyDocument214 pages2005 TJ BodyArt Doe100% (1)
- 02 Traps Management Service AdminDocument134 pages02 Traps Management Service AdminDonovan RuizNo ratings yet
- Ddal Players Guide v5Document12 pagesDdal Players Guide v5Jakob Cherpovsky100% (1)
- Data Management: Quantifying Data & Planning Your AnalysisDocument38 pagesData Management: Quantifying Data & Planning Your AnalysisSaqlain TariqNo ratings yet
- Three-Phase Induction MotorsDocument32 pagesThree-Phase Induction MotorsDimitriu CarmenNo ratings yet