You might also like
- Recurrent Pregnancy LossFrom EverandRecurrent Pregnancy LossOle Bjarne ChristiansenNo ratings yet
- Bemonc ChecklistDocument2 pagesBemonc Checklistkengyakkersss100% (1)
- Supportive Supervision Checklist For AFHCDocument5 pagesSupportive Supervision Checklist For AFHCDr. Ankur SangwanNo ratings yet
- Private Hospital New Format 12-09-23Document2 pagesPrivate Hospital New Format 12-09-23Rajendra HospitalNo ratings yet
- Antenatal CareDocument49 pagesAntenatal CareAyalewNo ratings yet
- Sentinel Event PolicyDocument6 pagesSentinel Event PolicyAnne Marjorie Futalan100% (1)
- Updated Abortion Statistics 2015Document89 pagesUpdated Abortion Statistics 2015Bruno ArllesNo ratings yet
- Sub Centre Level Monitoring Checklist PHC VisitDocument24 pagesSub Centre Level Monitoring Checklist PHC VisitVaish Navi100% (2)
- Supportive Supervision Plan & ChecklistsDocument50 pagesSupportive Supervision Plan & ChecklistsJennifer Pearson-Paredes100% (1)
- First-Trimester Bleeding: Advances in Family Practice NursingDocument13 pagesFirst-Trimester Bleeding: Advances in Family Practice NursingManuel MagañaNo ratings yet
- AMI - AbstPaperTool - V16.0a - ALPHADocument3 pagesAMI - AbstPaperTool - V16.0a - ALPHAHaritha AtluriNo ratings yet
- Assignment in NCM 211: Fhsis ComponentsDocument33 pagesAssignment in NCM 211: Fhsis ComponentsSheril Sularte CasanesNo ratings yet
- BC Centre For Disease Control: Tuberculosis ProgramDocument3 pagesBC Centre For Disease Control: Tuberculosis ProgramRoger DodgerNo ratings yet
- Comprehensive Reproductive Health Services Supervisory ChecklistDocument22 pagesComprehensive Reproductive Health Services Supervisory ChecklistMEKSELINA KALENDERNo ratings yet
- Texas Cancer Registry Cancer Reporting HandbookDocument37 pagesTexas Cancer Registry Cancer Reporting HandbookmagillaniNo ratings yet
- Annex e Hospital Stat Report Revised 7jan2014Document14 pagesAnnex e Hospital Stat Report Revised 7jan2014Andy Molina100% (1)
- Guidelines For SB and U5 Mortality Reporting System 2nd Edition 2018Document24 pagesGuidelines For SB and U5 Mortality Reporting System 2nd Edition 2018Roziha RahimNo ratings yet
- EKRA Maternal Health Program 1Document27 pagesEKRA Maternal Health Program 1Jerome CidNo ratings yet
- Breach PresentationDocument7 pagesBreach PresentationReema Akberali nooraniNo ratings yet
- 441 N Pos Ce Candidate GuidebookDocument23 pages441 N Pos Ce Candidate GuidebookVeronica ErlinNo ratings yet
- PCB Annexes A1-A5Document7 pagesPCB Annexes A1-A5Kleen Castro100% (4)
- Gena Family PlanningDocument14 pagesGena Family PlanningRuffa Jane Bangay RivasNo ratings yet
- Blood AdministrationDocument22 pagesBlood AdministrationJan-Michael R. RazoteNo ratings yet
- 2017 Annual Hospital QuestionnaireDocument23 pages2017 Annual Hospital QuestionnairebhagyaNo ratings yet
- Inguinal Hernia Repair ICP For WEBDocument16 pagesInguinal Hernia Repair ICP For WEBmarlinadewiNo ratings yet
- Maklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Document9 pagesMaklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Syazwi BaharuddinNo ratings yet
- Donor Selection and Blood CollectionDocument14 pagesDonor Selection and Blood CollectionMary ChristelleNo ratings yet
- DHIS Monthly Reporting Form (PHC Facilities)Document4 pagesDHIS Monthly Reporting Form (PHC Facilities)Usman88% (8)
- H Dip Fam Med (SA) Past Papers - 2016 2nd Semester 24-1-2017Document2 pagesH Dip Fam Med (SA) Past Papers - 2016 2nd Semester 24-1-2017matentenNo ratings yet
- Amebiasis: About The DiseaseDocument10 pagesAmebiasis: About The DiseaseBryan De HopeNo ratings yet
- Child Abuse 3Document9 pagesChild Abuse 3Nilsa RoblesNo ratings yet
- JointcommissionDocument27 pagesJointcommissionapi-245672784No ratings yet
- Notifiable Conditions FormDocument3 pagesNotifiable Conditions FormDarius DeeNo ratings yet
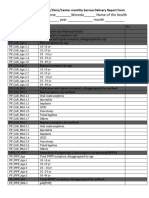
- DHIS Service Deliverey Report FormDocument25 pagesDHIS Service Deliverey Report FormAbreham BerhanNo ratings yet
- Bleeding and Pain in Early Pregnancy - RCOG PDFDocument4 pagesBleeding and Pain in Early Pregnancy - RCOG PDFSyandri Agus RizkyNo ratings yet
- Priniples of Obstetrical Referral To Tertiary Care CentreDocument32 pagesPriniples of Obstetrical Referral To Tertiary Care CentreNoorikiran HarisNo ratings yet
- Paediatric and Neonatal Service and Clinical Quality IndicatorsDocument8 pagesPaediatric and Neonatal Service and Clinical Quality IndicatorsSyamsul Arifin100% (1)
- PHC Karamtara Oct. 2015Document100 pagesPHC Karamtara Oct. 2015Ravi VaishnavNo ratings yet
- Q A 1Document48 pagesQ A 1ChannelGNo ratings yet
- Referral SystemDocument11 pagesReferral Systemabdul100% (1)
- Patient SafetyDocument22 pagesPatient SafetyRensy Sabi100% (1)
- Induced Termination of Pregnancy (ITOP) Reporting System GuideDocument36 pagesInduced Termination of Pregnancy (ITOP) Reporting System GuideYiddy Kester Vilchez ArellanosNo ratings yet
- Pre Transfusion Assessment Guidelines 2011Document3 pagesPre Transfusion Assessment Guidelines 2011zeinedNo ratings yet
- Case ScenarioDocument4 pagesCase ScenarioNaing Win Htet100% (1)
- Trauma PregnancyDocument19 pagesTrauma Pregnancyitsnaini indahNo ratings yet
- WCHGLM0021 Post Partum Haemorrhage Aug 2012Document13 pagesWCHGLM0021 Post Partum Haemorrhage Aug 2012bsbalfdfuagiludfhalkNo ratings yet
- Virtual Simulation 201 Clinical 1Document3 pagesVirtual Simulation 201 Clinical 1janaNo ratings yet
- National Health SituationDocument65 pagesNational Health SituationRegineNo ratings yet
- Reproductive Health IndicatorsDocument17 pagesReproductive Health IndicatorsRogers Talemwa WakefieldNo ratings yet
- Jurnal Plasenta PreviaDocument10 pagesJurnal Plasenta Previadiah_201192No ratings yet
- Components of HOPI FinalDocument2 pagesComponents of HOPI FinalkhanNo ratings yet
- Bates' Guide To Physical Examination and History Taking, 11th EditionDocument5 pagesBates' Guide To Physical Examination and History Taking, 11th EditionKitziaColliardNo ratings yet
- SOP RegionalDocument16 pagesSOP RegionalWilayah Strwberry-fizaNo ratings yet
- Tatalaksana Perdarahan ObstetriDocument10 pagesTatalaksana Perdarahan ObstetriAfiani JannahNo ratings yet
- Updated PGH Guidelines For ReferralsDocument2 pagesUpdated PGH Guidelines For ReferralsRocaya Lucman100% (1)
- ProtocolsDocument153 pagesProtocolsnutrientz100% (1)
- Navy Corpsman Sick Call Screeners GuideDocument215 pagesNavy Corpsman Sick Call Screeners GuidejustanothergunnutNo ratings yet
- Draft HC II, III, IV & V Workplan & Budget - Draft 0 - v7.6.2021Document26 pagesDraft HC II, III, IV & V Workplan & Budget - Draft 0 - v7.6.2021Joel ElemNo ratings yet
- Adverse Events Report 2012Document63 pagesAdverse Events Report 2012Mark BrackenburyNo ratings yet
- Pre-Registration Nursing Information For Prospective StudentsDocument4 pagesPre-Registration Nursing Information For Prospective StudentsbthangarajNo ratings yet
- Job Details Nts SNGPL 2018Document5 pagesJob Details Nts SNGPL 2018abuzaralmaniNo ratings yet
- Ppra McqsDocument8 pagesPpra McqsBEENANo ratings yet
- S.No. Designation Sanctioned Jul-18 Aug-18 Sep-18 Oct-18 Nov-18Document4 pagesS.No. Designation Sanctioned Jul-18 Aug-18 Sep-18 Oct-18 Nov-18Sohail AnjumNo ratings yet
- S.No. Designation Sanctioned Jul-18 Aug-18 Sep-18 Oct-18 Nov-18Document4 pagesS.No. Designation Sanctioned Jul-18 Aug-18 Sep-18 Oct-18 Nov-18Sohail AnjumNo ratings yet
- Nutrition InterventinDocument1 pageNutrition InterventinSohail AnjumNo ratings yet
- QuestionsDocument28 pagesQuestionssohail merchant100% (1)
- Term Finance CertificateDocument2 pagesTerm Finance CertificateSohail AnjumNo ratings yet
- What Is A Time SeriesDocument11 pagesWhat Is A Time SeriesSohail AnjumNo ratings yet
- Memorandum of AssociationDocument8 pagesMemorandum of AssociationSohail AnjumNo ratings yet
- Lay OutDocument1 pageLay OutSohail AnjumNo ratings yet
- Financial Statements Analysis: Presented byDocument40 pagesFinancial Statements Analysis: Presented bykakolalamamaNo ratings yet
- Sales Tax Act 1990 Updated Upto 2010Document84 pagesSales Tax Act 1990 Updated Upto 2010Sohail AnjumNo ratings yet
- DeiannieDocument11 pagesDeiannieapi-642218257No ratings yet
- 2020NRN - Perivascular Spaces in The Brain SUPPL PDFDocument2 pages2020NRN - Perivascular Spaces in The Brain SUPPL PDFJuan Carlos LazoNo ratings yet
- Food and Agricultural Import Regulations and Standards Country Report - Addis Ababa - Ethiopia - 12-31-2019Document20 pagesFood and Agricultural Import Regulations and Standards Country Report - Addis Ababa - Ethiopia - 12-31-2019Tesfaye NokoNo ratings yet
- Antenatal Care AduanaDocument36 pagesAntenatal Care AduanalaarnieNo ratings yet
- Depression Slides01 WhatisMajorDepressionDocument48 pagesDepression Slides01 WhatisMajorDepressionJohannes RebaneNo ratings yet
- Health Sectors Governing Health Care SystemDocument43 pagesHealth Sectors Governing Health Care SystemAyam Vale MallariNo ratings yet
- PMDC RulesDocument21 pagesPMDC RulesBabar Bashir85% (13)
- Funda Lec Midterm End ReviewerDocument39 pagesFunda Lec Midterm End ReviewerphoebeNo ratings yet
- Starting Med Guide 2019Document32 pagesStarting Med Guide 2019Benjamin AryaNo ratings yet
- PBCC PDFDocument1 pagePBCC PDFMaureen Dela ResmaNo ratings yet
- UK Art Therapy Practice-Based Guidelines For Children and Adults With Learning DisabilitiesDocument12 pagesUK Art Therapy Practice-Based Guidelines For Children and Adults With Learning DisabilitiesLNo ratings yet
- Telehealth Services: Target Audience: Medicare Fee-For-Service ProvidersDocument13 pagesTelehealth Services: Target Audience: Medicare Fee-For-Service ProvidersNataanatiNo ratings yet
- Webinar Perawatan Luka Dan Tata Laksana Pemeriksaan InfeksiDocument41 pagesWebinar Perawatan Luka Dan Tata Laksana Pemeriksaan Infeksiqoote3No ratings yet
- Slide Jurnal Efusi PleuraDocument8 pagesSlide Jurnal Efusi PleuraolakasturiNo ratings yet
- Interaction Process Analysis IpaDocument6 pagesInteraction Process Analysis Ipaapi-392699632No ratings yet
- MD GnewpDocument32 pagesMD GnewpVakeelVandumurugesanNo ratings yet
- Statement of Purpose: Why Ms in Pharmaceutical Science?Document2 pagesStatement of Purpose: Why Ms in Pharmaceutical Science?Khushwant Competitive Careers Pvt LtdNo ratings yet
- Brief Psychological Interventions PDFDocument6 pagesBrief Psychological Interventions PDFhema angleNo ratings yet
- NurseDocument12 pagesNurseanon-9626450% (2)
- Documentation Skills For Nursing Students.4Document6 pagesDocumentation Skills For Nursing Students.4BSN NyxNo ratings yet
- Health Care-Associated Infections - Best PracticesDocument9 pagesHealth Care-Associated Infections - Best PracticesJoshua DiaoNo ratings yet
- Thesis Sample Chapter 1Document5 pagesThesis Sample Chapter 1Romie SolacitoNo ratings yet
- ITI Decision Trees and ChecklistsDocument6 pagesITI Decision Trees and ChecklistsNay AungNo ratings yet
- General and Oral Pathology For Dental Hygiene PracticeDocument361 pagesGeneral and Oral Pathology For Dental Hygiene Practicepsychposters100% (1)
- Assessor Guide: Certification of Emergency Department in HospitalDocument11 pagesAssessor Guide: Certification of Emergency Department in Hospitalclab yuNo ratings yet
- Lecture-9 Therapeutics Planning: Pharmacy Practice ExperienceDocument19 pagesLecture-9 Therapeutics Planning: Pharmacy Practice ExperienceLayla100% (1)
- Global Perspectives On Mental HealthDocument21 pagesGlobal Perspectives On Mental Health4127297No ratings yet
- Declaration FormDocument1 pageDeclaration FormJzelNo ratings yet
- SALTAPSDocument24 pagesSALTAPSFatima Tu ZahraNo ratings yet
- 2011 3-17 Hendrickson Tables and References Re Post-Acute Growth Teaneck NJ Board of AdjustmentDocument7 pages2011 3-17 Hendrickson Tables and References Re Post-Acute Growth Teaneck NJ Board of AdjustmentLeslie HendricksonNo ratings yet