You might also like
- Limamg BisitaDocument1 pageLimamg BisitaJohn Lee Lorena GacusanNo ratings yet
- Prayer Before WorkDocument2 pagesPrayer Before WorkJohn Lee Lorena GacusanNo ratings yet
- Training of Trainers On 2013 Manual of Procedures of The NTP, 5 Edition Date: - Venue: - RationaleDocument5 pagesTraining of Trainers On 2013 Manual of Procedures of The NTP, 5 Edition Date: - Venue: - RationaleJohn Lee Lorena GacusanNo ratings yet
- The Anatomy of the Integumentary System: Skin's Two LayersDocument7 pagesThe Anatomy of the Integumentary System: Skin's Two LayersJohn Lee Lorena GacusanNo ratings yet
- Ra 7883Document3 pagesRa 7883John Lee Lorena GacusanNo ratings yet
- Complete Blood CountDocument10 pagesComplete Blood CountJohn Lee Lorena Gacusan100% (1)
- IMPACDocument186 pagesIMPACJohn Lee Lorena GacusanNo ratings yet
- The Cardiovascular SystemDocument21 pagesThe Cardiovascular SystemJohn Lee Lorena GacusanNo ratings yet
- RNHeals AppformDocument1 pageRNHeals AppformmarieNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
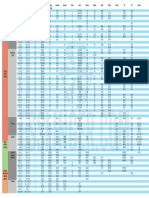
- Battery Cross Reference Chart - UnknownDocument1 pageBattery Cross Reference Chart - UnknownILikeScribd5050No ratings yet
- BEO Meeting GuidanceDocument20 pagesBEO Meeting Guidancesiput23100% (1)
- Workshop 19-10-23Document4 pagesWorkshop 19-10-23nathyoleasNo ratings yet
- Ede MicrprjctDocument21 pagesEde Micrprjct68 Nitesh PundgeNo ratings yet
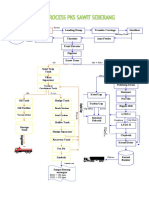
- 3 Skema Proses Pabrik Kelapa SawitDocument2 pages3 Skema Proses Pabrik Kelapa SawitWynne RaphaelaNo ratings yet
- 7 homemade organic pesticidesDocument3 pages7 homemade organic pesticidesWinssisNo ratings yet
- Simple Saraswati Homa: (1) Om Keśavāya Svāhā (2) Om Nārāya Āya Svāhā (3) Om Mādhavāya Svāhā OmDocument4 pagesSimple Saraswati Homa: (1) Om Keśavāya Svāhā (2) Om Nārāya Āya Svāhā (3) Om Mādhavāya Svāhā OmSoumava PalNo ratings yet
- Product 6Document5 pagesProduct 6TsabitaNo ratings yet
- ANCW30011 - Topic 7 ReadingsDocument41 pagesANCW30011 - Topic 7 ReadingsfaithNo ratings yet
- Phenylketonuria: Dietary Information For The Treatment ofDocument13 pagesPhenylketonuria: Dietary Information For The Treatment ofLuz Del ValleNo ratings yet
- Gcp1a Zambia Manuscript Art of MabisiDocument25 pagesGcp1a Zambia Manuscript Art of Mabisielizabeth haunduNo ratings yet
- 5 PsDocument14 pages5 PsNhật Anh PhạmNo ratings yet
- Hajj PKG 2024 - Labbaik HajjDocument5 pagesHajj PKG 2024 - Labbaik HajjAdil UsmaniNo ratings yet
- Investor - S Guide To The Care Economy - Four Dynamic Areas of Growth - July 2021Document266 pagesInvestor - S Guide To The Care Economy - Four Dynamic Areas of Growth - July 2021simyanliangNo ratings yet
- Barangay Profile of BulasaDocument6 pagesBarangay Profile of BulasaSharlene Mae DeiparineNo ratings yet
- Make It Easy!: BartendingDocument259 pagesMake It Easy!: BartendingObsessionNo ratings yet
- Kisi-Kisi Bing Answered 1-60Document12 pagesKisi-Kisi Bing Answered 1-60Rafli ApiNo ratings yet
- Soal PAT Kelas VIII - Bahasa InggrisDocument7 pagesSoal PAT Kelas VIII - Bahasa InggrisDavira Sandang OriNo ratings yet
- 40 Nov c114Document9 pages40 Nov c114bt20103120 Bharat SinghNo ratings yet
- Another Cup of CoffeeDocument86 pagesAnother Cup of CoffeeKarim ElouedNo ratings yet
- How A Man That Looks 20 at 50 Lives and What His Diet Is Like Bright SideDocument1 pageHow A Man That Looks 20 at 50 Lives and What His Diet Is Like Bright SideAmir AramNo ratings yet
- Math G5 Q1 WK2Document13 pagesMath G5 Q1 WK2MuhammadIshahaqBinBenjaminNo ratings yet
- Max Cafe Menu 2023Document2 pagesMax Cafe Menu 2023max.svjastinNo ratings yet
- Xavier University - Ateneo de CagayanDocument50 pagesXavier University - Ateneo de CagayanSheena AsahidNo ratings yet
- Gelatinized Sweet Potato Starches Obtained at Different Preheating Temperatures in A Spray DryerDocument8 pagesGelatinized Sweet Potato Starches Obtained at Different Preheating Temperatures in A Spray DryerThaís PaesNo ratings yet
- Count and Noncount NounsDocument3 pagesCount and Noncount NounsJorge GamaNo ratings yet
- IAF TC Meeting Minutes DraftDocument46 pagesIAF TC Meeting Minutes DraftArmand LiviuNo ratings yet
- Agroforestry As A Means of Alleviating Poverty in Sri LankaDocument7 pagesAgroforestry As A Means of Alleviating Poverty in Sri LankaArjuna SeneviratneNo ratings yet
- Report On MaFAAS Workshop and General Assembly 8 To 9 May 2013Document112 pagesReport On MaFAAS Workshop and General Assembly 8 To 9 May 2013Paul FatchNo ratings yet
- DEPORTEDocument108 pagesDEPORTEBritany Osorio MoranNo ratings yet