You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Body Systems (Grade 6) - Free Printable Tests and Worksheets - HelpTeachingDocument1 pageBody Systems (Grade 6) - Free Printable Tests and Worksheets - HelpTeachingshuganesh82% (11)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- U6C6 - Carty Soriano - Heart ValvesDocument6 pagesU6C6 - Carty Soriano - Heart ValvesXio LinaresNo ratings yet
- Pathology - Lab: Pathology of The Blood VesselsDocument5 pagesPathology - Lab: Pathology of The Blood VesselsRazel PerezNo ratings yet
- SLICC/ACR Damage Index GlossaryDocument1 pageSLICC/ACR Damage Index GlossarySilvana Chimá BustilloNo ratings yet
- Good BooksDocument16 pagesGood BooksFbihansip bancel100% (1)
- 5090 s09 QP 1Document20 pages5090 s09 QP 1wilsky05No ratings yet
- Fluid Mechanics of Blood CirculationDocument3 pagesFluid Mechanics of Blood CirculationChristian CustodioNo ratings yet
- Age-Reversing SecretDocument16 pagesAge-Reversing SecretRoosevelt KyleNo ratings yet
- 4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - SurgeryDocument60 pages4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - Surgeryqobsar100% (1)
- Harrison's 19e Cardiovascular SystemDocument7 pagesHarrison's 19e Cardiovascular SystemKarl CNo ratings yet
- Heart BlockDocument20 pagesHeart BlockSumathi GopinathNo ratings yet
- Cardio Quiz 2011Document4 pagesCardio Quiz 2011drifter191No ratings yet
- Ecg Presentation 2013Document40 pagesEcg Presentation 2013Samuel FpNo ratings yet
- ActivityDocument6 pagesActivityandreskalikasansaraNo ratings yet
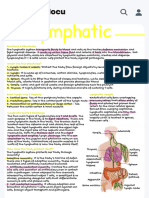
- Handwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuDocument1 pageHandwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuAllyssa MarieNo ratings yet
- St. Ignacia High School 1st Preliminary Exam in Science 10Document12 pagesSt. Ignacia High School 1st Preliminary Exam in Science 10Mira VeranoNo ratings yet
- DLL Science-6 Q2 W3Document6 pagesDLL Science-6 Q2 W3Grea Dela Cruz EdnilaoNo ratings yet
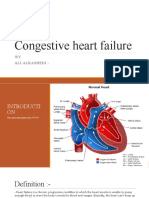
- CHF: Congestive Heart Failure Causes, Symptoms & TreatmentDocument13 pagesCHF: Congestive Heart Failure Causes, Symptoms & Treatmentali alrashediNo ratings yet
- Aortic RegurgitationDocument16 pagesAortic Regurgitationrobby zayendraNo ratings yet
- Left Anterior Fascicular Block (LAFB) - LITFL - ECG Library DiagnosisDocument1 pageLeft Anterior Fascicular Block (LAFB) - LITFL - ECG Library DiagnosisemmyNo ratings yet
- Paediatric Chest X-RayDocument10 pagesPaediatric Chest X-Raypheeplukz100% (1)
- Echocardiography ExaminationDocument10 pagesEchocardiography ExaminationYanira NoemíNo ratings yet
- FOE Graduate CatalogueDocument64 pagesFOE Graduate CatalogueMajed ImadNo ratings yet
- B. Pharm Syllabus 2014 Submitted To RGUHSDocument130 pagesB. Pharm Syllabus 2014 Submitted To RGUHSIbrahim GatarNo ratings yet
- Mark of Fitness Five Year Warranty: InstructionsDocument9 pagesMark of Fitness Five Year Warranty: InstructionsCoordinador MantenimientoNo ratings yet
- BODY FLUIDS AND CIRCULATION - DPP by Seep PahujaDocument49 pagesBODY FLUIDS AND CIRCULATION - DPP by Seep PahujahhNo ratings yet
- Lab 7 - Human PhysiologyDocument9 pagesLab 7 - Human Physiologyapi-383698554No ratings yet
- Description: Congestive Heart FailureDocument22 pagesDescription: Congestive Heart FailurePinklet Arleena CubianNo ratings yet
- Diagnosis: Imaging of Valvular Heart Disease in Heart FailureDocument9 pagesDiagnosis: Imaging of Valvular Heart Disease in Heart FailureAudini BerbasariNo ratings yet
- Klinik Farrali Medicare-ProfileDocument42 pagesKlinik Farrali Medicare-Profilemohd_noor_58No ratings yet