You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Cardio Vascular System NursingDocument2 pagesCardio Vascular System NursingGade BalajiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Chap. 18 GuytonDocument4 pagesChap. 18 GuytonMarian Joyce Princess Yuque100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Anatomy Quiz 2Document45 pagesAnatomy Quiz 2Upscaled100% (1)
- Life Processes 1Document36 pagesLife Processes 1Generic nameNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Cardiovascular System Summary Notes Vafum8Document9 pagesCardiovascular System Summary Notes Vafum8Taskeen BaberNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- ALL Clinicals of ThoraxDocument26 pagesALL Clinicals of Thoraxnaranjanlal01No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Mammalian HeartDocument7 pagesMammalian Heartnickmirad2No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- AQA As-Level Biology Revision Notes - New SpecDocument38 pagesAQA As-Level Biology Revision Notes - New SpecjimboNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grade 8 - 1st Monthly Exams - ScienceDocument23 pagesGrade 8 - 1st Monthly Exams - ScienceInah MasubayNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Unit 7-Common Diseases and Conditions of Body SystemsDocument227 pagesUnit 7-Common Diseases and Conditions of Body Systemstau88100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Human Anatomy,: First Edition Mckinley & O'LoughlinDocument65 pagesHuman Anatomy,: First Edition Mckinley & O'Loughlinİsmail ŞimşekNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Neonatal Transition: Training of The Trainers Neonatal ResuscitationDocument36 pagesNeonatal Transition: Training of The Trainers Neonatal ResuscitationmitaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Anatomy Heart and Great VesselsDocument54 pagesAnatomy Heart and Great VesselsRaviNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- For Printing Grand Case Group1Document37 pagesFor Printing Grand Case Group1Joco Bordeos AripNo ratings yet
- S9 Q4 M1 Transport and Excretion and Respiration and Energy Exchange QuizDocument3 pagesS9 Q4 M1 Transport and Excretion and Respiration and Energy Exchange QuizJermae DizonNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- First Periodical Test Science ViDocument4 pagesFirst Periodical Test Science ViHanzelkris CubianNo ratings yet
- Heart ImagesDocument74 pagesHeart ImagesNaveen EldoseNo ratings yet
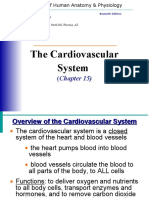
- The Cardiovascular System: (Chapter 15)Document59 pagesThe Cardiovascular System: (Chapter 15)Hasanuddin NuruNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Nutrients and Waste Transport SystemDocument22 pagesNutrients and Waste Transport SystemItsPotatoQueen MaeNo ratings yet
- Basics of Cath LabDocument121 pagesBasics of Cath LabizalxrayNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Nursing Care PlanDocument3 pagesNursing Care PlanBhie DizonNo ratings yet
- Gupta 2014Document145 pagesGupta 2014azmiNo ratings yet
- CH-11 Transportation in Animals and PlantsDocument12 pagesCH-11 Transportation in Animals and PlantsNaitik MeenaNo ratings yet
- Cardiovascular System - ReviewerDocument11 pagesCardiovascular System - ReviewerEva Marie GaaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Biology Notes For Unit 5Document84 pagesBiology Notes For Unit 5nhmerali7860% (1)
- Annicchiaricopetruzzelli Thesis 2017Document90 pagesAnnicchiaricopetruzzelli Thesis 2017Lia SantillanNo ratings yet
- Bor Kavcic: Electrodynamics of Human HeartDocument14 pagesBor Kavcic: Electrodynamics of Human HearttohunabohunNo ratings yet
- Critical Care NotesDocument18 pagesCritical Care NotesjulieNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Common OstrichDocument165 pagesCommon OstrichHarish BhatNo ratings yet
- Learners Material Module 1 Respiratory ADocument27 pagesLearners Material Module 1 Respiratory AJelly FloresNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)