You might also like
- In Vitro Bacterial Penetration of Coronally UnsealedDocument4 pagesIn Vitro Bacterial Penetration of Coronally UnsealedAlejandro Junior GarayNo ratings yet
- Intraorifice Sealing Ability of Different Materials in Endodontically Treated TeethDocument5 pagesIntraorifice Sealing Ability of Different Materials in Endodontically Treated TeethJing XueNo ratings yet
- Evaluation MTA and CaOH in Formation of Dentinal Bridge PDFDocument8 pagesEvaluation MTA and CaOH in Formation of Dentinal Bridge PDFRavik FidayatikaNo ratings yet
- Disinfection of Immature Teeth With A Triple Antibiotic PasteDocument5 pagesDisinfection of Immature Teeth With A Triple Antibiotic PasteMunish BatraNo ratings yet
- De-Deus, Leal, Soares - 2008 - Dye Extraction Results On Bacterial Leakproof Root Fillings G1Document3 pagesDe-Deus, Leal, Soares - 2008 - Dye Extraction Results On Bacterial Leakproof Root Fillings G1Latifah AFNo ratings yet
- Evaluation of Mineral Trioxide Aggregate (MTA) Versus Calcium Hydroxide Cement (Dycal ) in The Formation of A Dentine Bridge: A Randomised Controlled TrialDocument7 pagesEvaluation of Mineral Trioxide Aggregate (MTA) Versus Calcium Hydroxide Cement (Dycal ) in The Formation of A Dentine Bridge: A Randomised Controlled TrialCHOUCHOU12485No ratings yet
- Khayat - Human Saliva Penetration of Coronally Unsealed Obturated Root Canals-Journal of EndodonticsDocument4 pagesKhayat - Human Saliva Penetration of Coronally Unsealed Obturated Root Canals-Journal of Endodonticsadioos6767No ratings yet
- Journal Pre-ProofDocument23 pagesJournal Pre-ProofzaheerbdsNo ratings yet
- Comparative in Vivo Analysis of The Sealing Ability of Three Endodontic Sealers in Post-Prepared Root CanalsDocument7 pagesComparative in Vivo Analysis of The Sealing Ability of Three Endodontic Sealers in Post-Prepared Root CanalsCARLOSNo ratings yet
- Conde 2016Document16 pagesConde 2016TalesCamposNo ratings yet
- Artigo Original Artigo Original Artigo Original Artigo Original Artigo OriginalDocument5 pagesArtigo Original Artigo Original Artigo Original Artigo Original Artigo OriginalNida BuikaitėNo ratings yet
- Jioh 7 88Document6 pagesJioh 7 88aulia lubisNo ratings yet
- Takahashi 2009Document4 pagesTakahashi 2009IsabelleNo ratings yet
- The Prosthodontic Management of Endodontically Treated Teeth - A Literature Review. Part II. MaintDocument3 pagesThe Prosthodontic Management of Endodontically Treated Teeth - A Literature Review. Part II. MaintkochikaghochiNo ratings yet
- Effect of ProTaper Universal, Endoflare, Revo-S, HyFlexDocument3 pagesEffect of ProTaper Universal, Endoflare, Revo-S, HyFlexshamshuddin patelNo ratings yet
- Effect of Glass-Ionomer Cement As An Intra-Canal Barrier in Post Space Prepared Teeth: An in Vitro StudyDocument5 pagesEffect of Glass-Ionomer Cement As An Intra-Canal Barrier in Post Space Prepared Teeth: An in Vitro StudyVICTOR FERNANDO LAMAS LARANo ratings yet
- Preclinical Effectiveness of A Novel Pulp Capping MaterialDocument8 pagesPreclinical Effectiveness of A Novel Pulp Capping MaterialPatrícia LopesNo ratings yet
- Avaliação Da Difusão de Endotoxinas Através Dos Túbulos DentináriosDocument6 pagesAvaliação Da Difusão de Endotoxinas Através Dos Túbulos Dentináriosonurb90No ratings yet
- En Do Don TicsDocument5 pagesEn Do Don TicsAbhinav TalekarNo ratings yet
- Intracanal Medicament and ResilonDocument5 pagesIntracanal Medicament and ResilonLuLu NikhlaturNo ratings yet
- Single Visit Mta Apexification Technique For Formation of Root-End Barrier in Open Apices-A Case SeriesDocument7 pagesSingle Visit Mta Apexification Technique For Formation of Root-End Barrier in Open Apices-A Case Seriesdrvivek reddyNo ratings yet
- Mineral Trioxide Aggregate (MTA) and Calcium Hydroxide As Pulp-Capping Agents in Human Teeth: A Preliminary ReportDocument7 pagesMineral Trioxide Aggregate (MTA) and Calcium Hydroxide As Pulp-Capping Agents in Human Teeth: A Preliminary ReportMushidayah AuliaNo ratings yet
- Paper Pedo TrsnalteDocument15 pagesPaper Pedo TrsnaltecahayaNo ratings yet
- Effects of Sealant and Self Etching Primer On Enamel Decalcification. Part I An in Vitro StudyDocument7 pagesEffects of Sealant and Self Etching Primer On Enamel Decalcification. Part I An in Vitro Studyสุธีรพรรณ ทับแจ้งNo ratings yet
- Microbial Biofilm Proliferation Within Sealer-Root Dentin Interfaces Is Affected by Sealer Type and Aging PeriodDocument4 pagesMicrobial Biofilm Proliferation Within Sealer-Root Dentin Interfaces Is Affected by Sealer Type and Aging PeriodKapil JhajhariaNo ratings yet
- Apical Sealing Ability of MTA in Different Liquid To Powder Ratios and Packing MethodsDocument5 pagesApical Sealing Ability of MTA in Different Liquid To Powder Ratios and Packing MethodselnadaNo ratings yet
- Chen 2018Document5 pagesChen 2018hamada2751994No ratings yet
- Jurnal 5 - Cobankara2006Document3 pagesJurnal 5 - Cobankara2006Amelia RahmayantiNo ratings yet
- Comparison Between Gutta-Percha and Resilon Retreatment: Journal of Oral Science July 2009Document6 pagesComparison Between Gutta-Percha and Resilon Retreatment: Journal of Oral Science July 2009Thanh Minh NguyễnNo ratings yet
- 10 1016@j Joen 2013 07 034Document4 pages10 1016@j Joen 2013 07 034Asmita SonawneNo ratings yet
- Artigo EndoxDocument6 pagesArtigo EndoxSiti Harwati DesrimelinaNo ratings yet
- Three Methods of Obturation Using The Obtura II SystemDocument3 pagesThree Methods of Obturation Using The Obtura II SystemAnn M.No ratings yet
- Effect of Saliva Contamination On The Shear BondDocument5 pagesEffect of Saliva Contamination On The Shear BondHafaifa TaiebNo ratings yet
- The Effect of Different Final Irrigant Activation TechniquesDocument5 pagesThe Effect of Different Final Irrigant Activation TechniquesFrancisco liebbeNo ratings yet
- An Assessment of Microbial Coronal Leakage of Temporary Filling Materials in Endodontically Treated TeethDocument3 pagesAn Assessment of Microbial Coronal Leakage of Temporary Filling Materials in Endodontically Treated TeethsrinandanNo ratings yet
- Protaper PDFDocument5 pagesProtaper PDFWidhi Satrio NugrohoNo ratings yet
- The Effect of Calcium Hydroxide On The Short and Long-Term Sealing Properties of MTA Apical BarrierDocument5 pagesThe Effect of Calcium Hydroxide On The Short and Long-Term Sealing Properties of MTA Apical BarrierpoojaNo ratings yet
- Somma Et Al. 2011 (Quality of Thermoplasticized and Single Point Root) PDFDocument8 pagesSomma Et Al. 2011 (Quality of Thermoplasticized and Single Point Root) PDFCarla Itzel C SánchezNo ratings yet
- Root Canal Retreatment Using Reciprocating and Continuous Rotary Nickel-Titanium InstrumentsDocument7 pagesRoot Canal Retreatment Using Reciprocating and Continuous Rotary Nickel-Titanium InstrumentsralszNo ratings yet
- Laurell 1995 Bis PDFDocument12 pagesLaurell 1995 Bis PDFcis freteNo ratings yet
- Annual Review of Selected Scientific Literature 1Document36 pagesAnnual Review of Selected Scientific Literature 1abdulrar100% (1)
- Agitation Protocols in IrriDocument4 pagesAgitation Protocols in IrriAdriana Sorina SegărceanuNo ratings yet
- 13.bacterial Leakage in Root Canals Filled WithDocument6 pages13.bacterial Leakage in Root Canals Filled WithMihaela TuculinaNo ratings yet
- Bioabsorbable Root Analogue For Closure of Oroanatral Communication - Thoma Et Al - BIBL 36Document7 pagesBioabsorbable Root Analogue For Closure of Oroanatral Communication - Thoma Et Al - BIBL 36stoia_sebiNo ratings yet
- 08 - Apical and Periapical Tissues Responses After Root Canal Obturation With Two Calcium HydroxiDocument7 pages08 - Apical and Periapical Tissues Responses After Root Canal Obturation With Two Calcium Hydroxipkgarg_iitkgpNo ratings yet
- Influence of Sodium Hypochlorite and eDTA On The Microtensile Bond Strength of A Self-Etching Adhesive SystemDocument5 pagesInfluence of Sodium Hypochlorite and eDTA On The Microtensile Bond Strength of A Self-Etching Adhesive SystemDaniela Constanza CornejoNo ratings yet
- Influence of Cavity Type and Size of Composite Restorations On Cuspal FlexureDocument5 pagesInfluence of Cavity Type and Size of Composite Restorations On Cuspal FlexureAditi ChandraNo ratings yet
- Articulo Ahmad OOO ImpresoDocument4 pagesArticulo Ahmad OOO Impresoradamanthis 28No ratings yet
- 1.JCD Article 2013Document5 pages1.JCD Article 2013bhaskaracharya dontabhaktuniNo ratings yet
- Apically Extruded Sealers - Fate and Influence On Treatment Outcome 2016Document7 pagesApically Extruded Sealers - Fate and Influence On Treatment Outcome 2016Lorena CândidoNo ratings yet
- Dentistry Journal: Adhesion of Two New Glass Fiber Post Systems Cemented With Self-Adhesive Resin CementsDocument8 pagesDentistry Journal: Adhesion of Two New Glass Fiber Post Systems Cemented With Self-Adhesive Resin CementsDra. Fabiola BermudezNo ratings yet
- Dentistry Journal: Adhesion of Two New Glass Fiber Post Systems Cemented With Self-Adhesive Resin CementsDocument8 pagesDentistry Journal: Adhesion of Two New Glass Fiber Post Systems Cemented With Self-Adhesive Resin CementsDeisy Angarita FlorezNo ratings yet
- Determining The Optimal Length of The Tooth's Root Canal ObturationDocument7 pagesDetermining The Optimal Length of The Tooth's Root Canal ObturationBogdanNo ratings yet
- Evaluation of Fracture Resistance of Roots Obturated With Resilon and Thermoplasticized Gutta-Percha: An in Vitro StudyDocument5 pagesEvaluation of Fracture Resistance of Roots Obturated With Resilon and Thermoplasticized Gutta-Percha: An in Vitro StudySeema Karnwal DixitNo ratings yet
- WhiteandElezar CaOHweakeningdentinDocument3 pagesWhiteandElezar CaOHweakeningdentinJigar M. UpadhyayNo ratings yet
- Adhesion of Root Canal Selaers To DentinDocument6 pagesAdhesion of Root Canal Selaers To Dentinfun timesNo ratings yet
- A Histopathologic Study On Pulp Response To Glass Ionomer Cements in Human TeethDocument8 pagesA Histopathologic Study On Pulp Response To Glass Ionomer Cements in Human Teethnahm17No ratings yet
- CPP Acp ArticleDocument5 pagesCPP Acp ArticleDion KristamtomoNo ratings yet
- Minimally Invasive Approaches in Endodontic PracticeFrom EverandMinimally Invasive Approaches in Endodontic PracticeGianluca PlotinoNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Ijid D 19 00050 PDFDocument27 pagesIjid D 19 00050 PDFNeamat Hassan Abu-bakrNo ratings yet
- Jos (4) 2013Document9 pagesJos (4) 2013Neamat Hassan Abu-bakrNo ratings yet
- Ceramic CrownDocument5 pagesCeramic CrownNeamat Hassan Abu-bakrNo ratings yet
- Impression Materials: Dr. Neamat Hassan Abu-Bakr, BDS, Dss (Austria), MDSC (Scotland), PHD (Japan)Document85 pagesImpression Materials: Dr. Neamat Hassan Abu-Bakr, BDS, Dss (Austria), MDSC (Scotland), PHD (Japan)Neamat Hassan Abu-bakrNo ratings yet
- Management & B RDocument20 pagesManagement & B RNeamat Hassan Abu-bakrNo ratings yet
- 27-2 Summer 2011 PDFDocument132 pages27-2 Summer 2011 PDFBJ VeuxNo ratings yet
- Review Dentin Root DamageDocument4 pagesReview Dentin Root DamageHarry ArdiyantoNo ratings yet
- Clinical Classification of The Status of The Pulp and Dental HealthDocument15 pagesClinical Classification of The Status of The Pulp and Dental HealthrahaazadNo ratings yet
- Electric Pulp Testing: A ReviewDocument10 pagesElectric Pulp Testing: A ReviewWilliam BarrettNo ratings yet
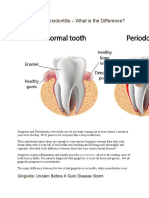
- Gingivitis Vs PeriodontitisDocument2 pagesGingivitis Vs Periodontitisandreas kevinNo ratings yet
- Occlusal Equilibration Between Option and Clinical RealtyDocument7 pagesOcclusal Equilibration Between Option and Clinical RealtyNanooa NanooaNo ratings yet
- Complete CPITN PRESENTATIONDocument16 pagesComplete CPITN PRESENTATIONDr. Zohaib AhmedNo ratings yet
- Evolution of Treatment Mechanics PDFDocument9 pagesEvolution of Treatment Mechanics PDFJunaid Israr - OrthodonticsNo ratings yet
- Molar DistalizationDocument26 pagesMolar DistalizationNeeraj AroraNo ratings yet
- Tongue Thrust and Braces: A Question and Answer GuideDocument2 pagesTongue Thrust and Braces: A Question and Answer GuideghyonasNo ratings yet
- Hall Technique, Stepwise Excavation, Partial Caries Removal TechniqueDocument4 pagesHall Technique, Stepwise Excavation, Partial Caries Removal TechniqueImbador LiesiesNo ratings yet
- Impression Techniques: For Implant ProsthesesDocument38 pagesImpression Techniques: For Implant Prosthesesbaqer hussain0% (1)
- Effects of Activator and High Pull Headgear Combination Therapy PDFDocument9 pagesEffects of Activator and High Pull Headgear Combination Therapy PDFDilesh PradhanNo ratings yet
- Rotation of Jaws During Growth and Maturational and Aging ChangesDocument15 pagesRotation of Jaws During Growth and Maturational and Aging Changesshahzeb memon100% (1)
- Indirect Bonding: A Comprehensive Review of The Advantages: Clinical Adv ANT Ages Improved Patient ComfortDocument7 pagesIndirect Bonding: A Comprehensive Review of The Advantages: Clinical Adv ANT Ages Improved Patient ComfortSyed LateefNo ratings yet
- Herbst ApplianceDocument36 pagesHerbst ApplianceSakthi Priya100% (5)
- Combination Syndrom: Dr. Farzana Memon Assistant Professor Dept. of Prosthodontics, Isra Dental College HyderabadDocument21 pagesCombination Syndrom: Dr. Farzana Memon Assistant Professor Dept. of Prosthodontics, Isra Dental College HyderabadLaiba Asif RajputNo ratings yet
- Furcation Involvement and ManagementDocument9 pagesFurcation Involvement and ManagementrubaNo ratings yet
- Endocrown Review 1Document9 pagesEndocrown Review 1Anjali SatsangiNo ratings yet
- Utility ArchesDocument2 pagesUtility ArchesDevanand Gupta67% (3)
- Bone Loss PatternsDocument36 pagesBone Loss PatternsMavis100% (1)
- Fractured Root Tips During Dental Extractions and Retained Root Fragments. A Clinical Dilemma?Document7 pagesFractured Root Tips During Dental Extractions and Retained Root Fragments. A Clinical Dilemma?Siti Ulfah NesiaNo ratings yet
- Cast Gold InlaysDocument20 pagesCast Gold InlaysGayathriNo ratings yet
- Lingualized Occlusion ReviewDocument3 pagesLingualized Occlusion ReviewJessy ChenNo ratings yet
- 1.miu - Orthodontics For Undergtaduate 6th Edition On CDDocument219 pages1.miu - Orthodontics For Undergtaduate 6th Edition On CDahmedsyNo ratings yet
- article-pdf-RAJEEV GUPTA ARCHANA NAGPAL SUKHRAJ SINGH SAINI VI-689 PDFDocument5 pagesarticle-pdf-RAJEEV GUPTA ARCHANA NAGPAL SUKHRAJ SINGH SAINI VI-689 PDFKrupali JainNo ratings yet
- Tips On Tooth Preparation For C&BDocument8 pagesTips On Tooth Preparation For C&Bizeldien5870No ratings yet
- Gingival Overgrowth and Altered Passive Eruption in Adolescents Literature Review and Case ReportDocument8 pagesGingival Overgrowth and Altered Passive Eruption in Adolescents Literature Review and Case ReportAulia ElnisaNo ratings yet
- Operative Cba 2Document3 pagesOperative Cba 2AsmaNo ratings yet
- Anterior Teeth SelectionDocument83 pagesAnterior Teeth SelectionAysha Mohammedali100% (2)