You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 5.2.3 Piling WorksDocument12 pages5.2.3 Piling WorksPaul KwongNo ratings yet
- 5.1 Architectural Material SpecificationDocument4 pages5.1 Architectural Material SpecificationPaul Kwong100% (1)
- Conopy & Passge WayDocument5 pagesConopy & Passge WayPaul KwongNo ratings yet
- Construction and Infrastructure Developments in Myanmar Feb 2014Document3 pagesConstruction and Infrastructure Developments in Myanmar Feb 2014Paul KwongNo ratings yet
- Myanmar Capital Gains Tax Rates, and Property Income TaxDocument8 pagesMyanmar Capital Gains Tax Rates, and Property Income TaxPaul KwongNo ratings yet
- Tender Presentation: Qingjian International (Myanmar) Group Development Co., LTDDocument1 pageTender Presentation: Qingjian International (Myanmar) Group Development Co., LTDPaul KwongNo ratings yet
- YCDC Notification No 9 1999Document16 pagesYCDC Notification No 9 1999Paul KwongNo ratings yet
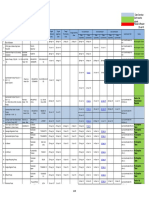
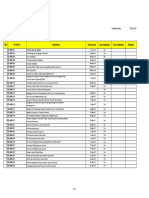
- Date Over-Due Don't Need To Submit Revise & Resubmit M&E Shop Drawing Register Combine Service Drawing & Structural Electrical and Mechanical Drawing (CSD & SEM) Updated Date: 25-Jul-15Document36 pagesDate Over-Due Don't Need To Submit Revise & Resubmit M&E Shop Drawing Register Combine Service Drawing & Structural Electrical and Mechanical Drawing (CSD & SEM) Updated Date: 25-Jul-15Paul KwongNo ratings yet
- Material Catalogue Submission List (19-Aug-15)Document1 pageMaterial Catalogue Submission List (19-Aug-15)Paul KwongNo ratings yet
- Shop Drawings Submission List (6-Aug-15)Document3 pagesShop Drawings Submission List (6-Aug-15)Paul KwongNo ratings yet
- RfiDocument5 pagesRfiPaul KwongNo ratings yet
- Material Catalogue Submission List (6-Aug-15)Document2 pagesMaterial Catalogue Submission List (6-Aug-15)Paul KwongNo ratings yet
- MfaDocument26 pagesMfaPaul KwongNo ratings yet
- Updated Date: 25-Jul-15 M&E EI Register List From Alpha S/N EI Ref No. Description Date Issued Cost Implication Time Implication RemarksDocument2 pagesUpdated Date: 25-Jul-15 M&E EI Register List From Alpha S/N EI Ref No. Description Date Issued Cost Implication Time Implication RemarksPaul KwongNo ratings yet
- 1708-2308 MANPOWER (22 Aug 15)Document2 pages1708-2308 MANPOWER (22 Aug 15)Paul KwongNo ratings yet
- DATE: 17 23-Aug-15 Daily Man Power Progress Report For M&E System at Sule Square ProjectDocument2 pagesDATE: 17 23-Aug-15 Daily Man Power Progress Report For M&E System at Sule Square ProjectPaul KwongNo ratings yet
- Ed M&e 001 Ed M&e 002 Ed M&e 003 Ed M&e 004 Ed M&e 005 Ed M&e 006 Ed M&e 007 Ed M&e 008Document1 pageEd M&e 001 Ed M&e 002 Ed M&e 003 Ed M&e 004 Ed M&e 005 Ed M&e 006 Ed M&e 007 Ed M&e 008Paul KwongNo ratings yet
- 1708-2308 MANPOWER (21 Aug 15)Document1 page1708-2308 MANPOWER (21 Aug 15)Paul KwongNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hotel Supervision IndividualDocument6 pagesHotel Supervision IndividualMohd YusufNo ratings yet
- MS03 09 Capital Budgeting Part 1 EncryptedDocument8 pagesMS03 09 Capital Budgeting Part 1 EncryptedKate Crystel reyesNo ratings yet
- Tax 1 CorpDocument16 pagesTax 1 CorpRen A Eleponio0% (1)
- List of Mncs in BangladeshDocument60 pagesList of Mncs in BangladeshAshiaNo ratings yet
- A Project Report On HDFC BankDocument45 pagesA Project Report On HDFC BankMukesh LalNo ratings yet
- Transnet Annual Report 2003 - 2004Document126 pagesTransnet Annual Report 2003 - 2004cameroonwebnewsNo ratings yet
- Sales Management: 1 Compiled by T S Dawar - Sales Management Lecture 7 & 8Document21 pagesSales Management: 1 Compiled by T S Dawar - Sales Management Lecture 7 & 8sagartolaneyNo ratings yet
- Capital & RevenueDocument7 pagesCapital & RevenueDr Sarbesh Mishra50% (2)
- Islamic Finance and Their Financial Growth Verses Their Maqasid Al ShariahDocument54 pagesIslamic Finance and Their Financial Growth Verses Their Maqasid Al ShariahNader MehdawiNo ratings yet
- Capital BudgetingDocument53 pagesCapital BudgetingSaahil LedwaniNo ratings yet
- Government Accountability Office - Ensuring Income Throughout Retirement Requires Difficult ChoicesDocument79 pagesGovernment Accountability Office - Ensuring Income Throughout Retirement Requires Difficult ChoicesEphraim DavisNo ratings yet
- Intraday Trend: Maruti SpotDocument18 pagesIntraday Trend: Maruti Spothoney1002No ratings yet
- 2017 Annual Report KiaDocument74 pages2017 Annual Report Kiakavitha kalasudhanNo ratings yet
- Project Report On Banking Sector Stocks by Using Technical AnalysisDocument12 pagesProject Report On Banking Sector Stocks by Using Technical Analysisaurorashiva167% (3)
- Syllabus Personal FinanceDocument23 pagesSyllabus Personal FinanceShahanie Joy Reyes50% (4)
- V1 Exam 1AMDocument19 pagesV1 Exam 1AMatmankhaiNo ratings yet
- Quiz BeeDocument15 pagesQuiz BeeRudolf Christian Oliveras UgmaNo ratings yet
- Deaths Accidents and Other Mishaps at Bukit Tabur - Astro AwaniDocument6 pagesDeaths Accidents and Other Mishaps at Bukit Tabur - Astro AwaniNur FithriyaniNo ratings yet
- J&L RailroadDocument6 pagesJ&L RailroadRichard Emanuel100% (1)
- Principles and Practices of BankingDocument63 pagesPrinciples and Practices of BankingPaavni SharmaNo ratings yet
- Washington Mutual, Inc 8k 20111216Document578 pagesWashington Mutual, Inc 8k 20111216emily523No ratings yet
- Financial Feasibility Study 2020/2021: Theoretical PartDocument17 pagesFinancial Feasibility Study 2020/2021: Theoretical Partislam hamdyNo ratings yet
- Independent University, Bangladesh.: Course Code: ACN-305Document19 pagesIndependent University, Bangladesh.: Course Code: ACN-305Ahsanur Hossain Tonmoy100% (1)
- Brown, Walter W. or Annabelle P. BrownDocument20 pagesBrown, Walter W. or Annabelle P. BrownJan Ellard CruzNo ratings yet
- Balance Sheet: Notes 2010 Taka 2009 TakaDocument5 pagesBalance Sheet: Notes 2010 Taka 2009 TakaThushara SilvaNo ratings yet
- Responsibility Acctg, Transfer Pricing & GP AnalysisDocument22 pagesResponsibility Acctg, Transfer Pricing & GP Analysisboen jayme50% (2)
- Thesis Islamic BankinglDocument164 pagesThesis Islamic BankinglZaib NawazNo ratings yet
- International Journal of Economic Practices and TheoriesDocument14 pagesInternational Journal of Economic Practices and TheoriesElena PradaNo ratings yet
- Accounting Concepts and ConventionsDocument2 pagesAccounting Concepts and ConventionsBhagya FernandoNo ratings yet
- Snap Fitness Franchise OpportunityDocument7 pagesSnap Fitness Franchise OpportunityrtphockjockNo ratings yet