You might also like
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Electrocardiograph Y: Dr. Fatimah Eliana, SPPD, Kemd, FinasimDocument118 pagesElectrocardiograph Y: Dr. Fatimah Eliana, SPPD, Kemd, FinasimTommy WidjayaNo ratings yet
- Definition ECGDocument8 pagesDefinition ECGMelody BoadoNo ratings yet
- Atrial Flutter: The Lancet Carotid Sinus MassageDocument3 pagesAtrial Flutter: The Lancet Carotid Sinus Massageyosi rizalNo ratings yet
- Chapter 5: Analyzing A Rhythm StripDocument7 pagesChapter 5: Analyzing A Rhythm StriptellyNo ratings yet
- ECG InterpretationDocument11 pagesECG InterpretationAndrea AndradaNo ratings yet
- Supraventricular TachycardiaDocument9 pagesSupraventricular TachycardiaclubsanatateNo ratings yet
- EKG InterpretationDocument63 pagesEKG InterpretationMiriam Cindy MathullaNo ratings yet
- Ventricular Sense ResponseDocument3 pagesVentricular Sense ResponseDaniel Banina AguerreNo ratings yet
- Atrial RhythmDocument12 pagesAtrial RhythmCarlo Domingo LadieroNo ratings yet
- ECG InterpretationDocument1 pageECG InterpretationCecil-An DalanonNo ratings yet
- Common Arrhythmias - The Importance of ECG InterpretationDocument9 pagesCommon Arrhythmias - The Importance of ECG InterpretationDANIELA PARRA GARCIANo ratings yet
- ECG Interpretation (WSAVA 2007, Boswood)Document5 pagesECG Interpretation (WSAVA 2007, Boswood)Kevin ChoyNo ratings yet
- How To Read An ECGDocument21 pagesHow To Read An ECGSlychenkoNo ratings yet
- Abnomalites of ECGDocument81 pagesAbnomalites of ECGgrreddy8364320No ratings yet
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- Ecg WorkshopDocument39 pagesEcg WorkshopUber SnooferNo ratings yet
- How To Read An ECGDocument15 pagesHow To Read An ECGcharlyn206No ratings yet
- How To Read An ECG: Confirm DetailsDocument15 pagesHow To Read An ECG: Confirm DetailsRinothja RajaratnamNo ratings yet
- ECG Interpretation For ACLSDocument27 pagesECG Interpretation For ACLSZH. omg sarNo ratings yet
- Ekg NetDocument15 pagesEkg NetDewi AyuNo ratings yet
- How To Read An ECGDocument15 pagesHow To Read An ECGSarah RonquilloNo ratings yet
- ECG StudyDocument32 pagesECG StudyDan Daniel XuNo ratings yet
- Ipd Kuliah Ekg Blok KegawatdaruratanDocument118 pagesIpd Kuliah Ekg Blok Kegawatdaruratansiti solikhaNo ratings yet
- Electrocardiogram (ECG/EKG) : Jovel Balaba Tangonan InstructorDocument77 pagesElectrocardiogram (ECG/EKG) : Jovel Balaba Tangonan InstructorNecky AlbaciteNo ratings yet
- Kamis 10 September 2015 - IPD 2 - Kuliah-Ekg-Blok-KegawatdaruratanDocument118 pagesKamis 10 September 2015 - IPD 2 - Kuliah-Ekg-Blok-KegawatdaruratanIrfanArifZulfikarNo ratings yet
- Click Here To View: 3. Atrial Fibrillation (A-Fib)Document1 pageClick Here To View: 3. Atrial Fibrillation (A-Fib)Lwin Maung Maung ThikeNo ratings yet
- ECG MonitoringDocument96 pagesECG MonitoringJey BautistaNo ratings yet
- ECG InterpretationDocument52 pagesECG InterpretationMarcus, RN98% (44)
- A. Flutter, AFDocument80 pagesA. Flutter, AFclaimstudent3515No ratings yet
- ECG For BeginnersDocument61 pagesECG For Beginnersblndffl100% (2)
- Clinical Teaching Ecg InterpretationDocument25 pagesClinical Teaching Ecg InterpretationAnusha VergheseNo ratings yet
- Sally Aburumman Bushra SaleemDocument75 pagesSally Aburumman Bushra SaleemAbdulrahman AlsayyedNo ratings yet
- Atrial Flutter EmedicineDocument8 pagesAtrial Flutter EmedicineErnis Wahyu OktianaNo ratings yet
- Supraventricular TachycardiaDocument5 pagesSupraventricular TachycardialjubodragNo ratings yet
- Aritmii EngDocument90 pagesAritmii EngAnna HaritonencoNo ratings yet
- Basics of EKG InterpretationDocument132 pagesBasics of EKG InterpretationArif Imam HidayatNo ratings yet
- Ecg in Emergency: Adi SulistyantoDocument41 pagesEcg in Emergency: Adi Sulistyantomech_pilot2203No ratings yet
- Cardiac Arrhythmias: Group 3ADocument39 pagesCardiac Arrhythmias: Group 3AAradhanaRamchandaniNo ratings yet
- Cheong Kuan Loong Medical Department Hospital Sultan Haji Ahmad Shah, Temerloh 12/5/10Document99 pagesCheong Kuan Loong Medical Department Hospital Sultan Haji Ahmad Shah, Temerloh 12/5/10Haq10No ratings yet
- The Main Applications of The ECG Nursing Lecture NotesDocument19 pagesThe Main Applications of The ECG Nursing Lecture NotesMaria Rowena O. SalvoNo ratings yet
- How To Read An ECGDocument24 pagesHow To Read An ECGredroseeeeeeNo ratings yet
- ECG Tutorial - Basic Principles of ECG Analysis - UpToDateDocument17 pagesECG Tutorial - Basic Principles of ECG Analysis - UpToDateImja94No ratings yet
- DR Amao Core Principles of Interpreting Ecg TracingDocument39 pagesDR Amao Core Principles of Interpreting Ecg Tracingdan ekelemeNo ratings yet
- KalaiDocument47 pagesKalaiArya VikneshNo ratings yet
- Supraventricular Tachycardia - Life in The Fast Lane ECG LibraryDocument29 pagesSupraventricular Tachycardia - Life in The Fast Lane ECG LibraryYehuda Agus SantosoNo ratings yet
- 5 Steps To Rhythm Strip InterpretationDocument2 pages5 Steps To Rhythm Strip Interpretationjosh082572No ratings yet
- Basics of EKG InterpretationDocument53 pagesBasics of EKG InterpretationHala BahaaNo ratings yet
- Cardiac Arrhythmia 171209212142 2Document74 pagesCardiac Arrhythmia 171209212142 2Gunel Sadiqova100% (1)
- Marathon-Related ECG ExasperationDocument24 pagesMarathon-Related ECG ExasperationmohamedsmnNo ratings yet
- ECG Rhythm InterpretationDocument16 pagesECG Rhythm InterpretationJanettNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasFrom EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasRating: 3 out of 5 stars3/5 (5)
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- 2020 ESC Guidelines For The Management of Adult Congenital Heart Disease (Previously Grown-Up Congenital Heart Disease)Document84 pages2020 ESC Guidelines For The Management of Adult Congenital Heart Disease (Previously Grown-Up Congenital Heart Disease)Liliana BrochadoNo ratings yet
- CG B Ook: Rapid FindDocument25 pagesCG B Ook: Rapid FinddellaNo ratings yet
- PS410Inst Eng PDFDocument26 pagesPS410Inst Eng PDFfuadhalimNo ratings yet
- Ventricular FibrillationDocument6 pagesVentricular FibrillationclubsanatateNo ratings yet
- Quiz 2Document7 pagesQuiz 2fatiNo ratings yet
- ECG, EEG &, EMG: 45 Notes To PGDocument6 pagesECG, EEG &, EMG: 45 Notes To PGskycall28No ratings yet
- Internal Med Board Review Course BK 2013-2014Document564 pagesInternal Med Board Review Course BK 2013-2014Akash Bhatnagar100% (1)
- AGENDA ACARA FixDocument4 pagesAGENDA ACARA FixIra MashadiNo ratings yet
- Electrocardiography: ECG StandardizationDocument4 pagesElectrocardiography: ECG StandardizationRayan OlivaNo ratings yet
- Pathology+101 Complete)Document147 pagesPathology+101 Complete)Goh Kah Yong100% (2)
- Valvular Heart DiseaseDocument33 pagesValvular Heart Diseasesimran kaurNo ratings yet
- Cardio 7.4Document2 pagesCardio 7.4Абдул Насер МохаммадізмаелNo ratings yet
- Treadmill Test: Khairul Nizam Abdul Rahman 4262143008Document12 pagesTreadmill Test: Khairul Nizam Abdul Rahman 4262143008Dea Amelia YolandaNo ratings yet
- CardiomegalyDocument31 pagesCardiomegalyDeepika LingamNo ratings yet
- Answers MediDocument443 pagesAnswers MediAmine Younis100% (13)
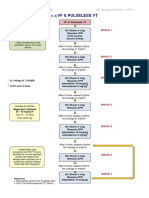
- VF & Pulseless VTDocument1 pageVF & Pulseless VTmadimadi11No ratings yet
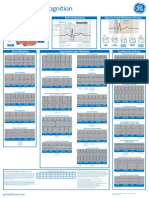
- Arrhythmia Recognition Part 1 and 2 DOC1178264 Rev2Document2 pagesArrhythmia Recognition Part 1 and 2 DOC1178264 Rev2Nico Angelo CopoNo ratings yet
- ECG Master Class-1Document132 pagesECG Master Class-1Shohag ID Center100% (1)
- Holter MonitoringDocument19 pagesHolter Monitoringomotola Ayobundle-oyewo MA206100% (1)
- Updated How To Deal ACS in Limited Resources Facilities - Danie Syahrir, DR., SP - JPDocument32 pagesUpdated How To Deal ACS in Limited Resources Facilities - Danie Syahrir, DR., SP - JPmaria sintaNo ratings yet
- Fuster Et Al 2001 Acc Aha Esc Guidelines For The Management of Patients With Atrial Fibrillation Executive Summary ADocument33 pagesFuster Et Al 2001 Acc Aha Esc Guidelines For The Management of Patients With Atrial Fibrillation Executive Summary AAlfita RahmawatiNo ratings yet
- Ecg - AclsDocument338 pagesEcg - AclsPete Cobra CobraitiNo ratings yet
- Capstone PPDocument20 pagesCapstone PPapi-569838480No ratings yet
- Claves de Cardiologia CX Cardiovascular VillamedicDocument0 pagesClaves de Cardiologia CX Cardiovascular VillamedicWendy Samaniego MojicaNo ratings yet
- Normal Sinus RhythmDocument10 pagesNormal Sinus RhythmNakul GaurNo ratings yet
- ECG For ACLS ModifiedDocument48 pagesECG For ACLS ModifiedIamnurse Nylej100% (1)
- Guias Hipertension 2023 Esc BDocument14 pagesGuias Hipertension 2023 Esc Bmiguel contrerasNo ratings yet
- Cardiovascular Examination IBDDocument6 pagesCardiovascular Examination IBDTRINIDAD, ALYANNA V.No ratings yet
- Sources: CardiovascularDocument117 pagesSources: CardiovascularMohannad AlfadhalNo ratings yet
- Congestive Heart Failure PDFDocument49 pagesCongestive Heart Failure PDFVerinice NañascaNo ratings yet