You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- REFERAT Koass Neurologi - Carpal Tunnel SyndromeDocument34 pagesREFERAT Koass Neurologi - Carpal Tunnel SyndromeVindhita RatiputriNo ratings yet
- InserviceDocument27 pagesInserviceapi-216088427No ratings yet
- Sports Injuries 1Document64 pagesSports Injuries 1Iulia Moldovan100% (1)
- Starting The Diagnose: Chakra Stone Massage 1Document14 pagesStarting The Diagnose: Chakra Stone Massage 1Kristal KrisNo ratings yet
- Physical Therapy in Sport: Robert Manske, Daniel ProhaskabDocument12 pagesPhysical Therapy in Sport: Robert Manske, Daniel ProhaskabLucaNo ratings yet
- Men's Health - Total Body WorkoutDocument28 pagesMen's Health - Total Body WorkoutQuim100% (1)
- Pencegahan Terjadinya Resiko Pengguna Nova Relida Samosir, Ayu Permata, Siti MuawanahDocument8 pagesPencegahan Terjadinya Resiko Pengguna Nova Relida Samosir, Ayu Permata, Siti MuawanahQusay ekzaNo ratings yet
- Cat Muscles and O.I.A.: Body Region Muscle Origin Insertion ActionDocument5 pagesCat Muscles and O.I.A.: Body Region Muscle Origin Insertion ActioneumarasiganNo ratings yet
- Range of Joint Motion Evaluation Chart: 1. Back 2. Lateral (Flexion)Document2 pagesRange of Joint Motion Evaluation Chart: 1. Back 2. Lateral (Flexion)JulesNo ratings yet
- Mišići Ruke - Mišići Ramenog Pojasa - Prednja StranaDocument14 pagesMišići Ruke - Mišići Ramenog Pojasa - Prednja StranaFanserbia100% (1)
- TFCC PDFDocument22 pagesTFCC PDFMayor AnakNo ratings yet
- Upper Limb OrthosisDocument84 pagesUpper Limb OrthosisShriyaNo ratings yet
- Jaspal R Singh, M.D.: Department of Rehabilitation MedicineDocument2 pagesJaspal R Singh, M.D.: Department of Rehabilitation MedicineshikhaNo ratings yet
- A&P - Muscle WorksheetDocument4 pagesA&P - Muscle WorksheetJerry GNo ratings yet
- ST - Mapeh 6 - Q2Document5 pagesST - Mapeh 6 - Q2Cherry Mae CaranzaNo ratings yet
- Eponymous Fractures 2Document48 pagesEponymous Fractures 2Sllavko K. KallfaNo ratings yet
- Joint Movements From Manual of Structural KinesiologyDocument7 pagesJoint Movements From Manual of Structural KinesiologyAlice GiffordNo ratings yet
- Sword & Scoundrel - Print Character Sheet v1.0.0bDocument2 pagesSword & Scoundrel - Print Character Sheet v1.0.0bAzalnubizarNo ratings yet
- (2P2) GROUP 2 - MusclesDocument5 pages(2P2) GROUP 2 - MusclesAlexa AurellanoNo ratings yet
- Rotator Cuff Isometric Exercises in Combination With Scapular MuscleDocument6 pagesRotator Cuff Isometric Exercises in Combination With Scapular MusclefilipecorsairNo ratings yet
- Fracture of Radius and Ulna 3Document38 pagesFracture of Radius and Ulna 3Noor Al Zahraa AliNo ratings yet
- Fingerprint 101Document10 pagesFingerprint 101Revier NasgadaNo ratings yet
- Assistive Devices: Roel B. Del Rosario, PTRPDocument63 pagesAssistive Devices: Roel B. Del Rosario, PTRPangel bolfriNo ratings yet
- OsteologyDocument96 pagesOsteologyBenita Putri MD100% (2)
- Bodybuilding AnatomyDocument188 pagesBodybuilding AnatomyLynseyNo ratings yet
- Bosco Arms & ShouldersDocument25 pagesBosco Arms & Shouldersmark.mcguigan992100% (3)
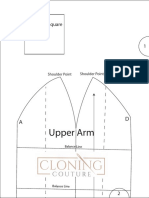
- Upper Arm: 2 Inch Test SquareDocument7 pagesUpper Arm: 2 Inch Test SquareMarcela RosalesNo ratings yet
- Kuki HanbojutsuDocument5 pagesKuki HanbojutsuphyllobiusNo ratings yet
- Musculoskeletal Imaging 2015Document79 pagesMusculoskeletal Imaging 2015Faiq Syukri Bin SaparudinNo ratings yet
- PROPER HANDWASHING ScriptDocument1 pagePROPER HANDWASHING ScriptJin morarengNo ratings yet