You might also like
- Pharm Expansion 17 NDFDocument1 pagePharm Expansion 17 NDFNokz M. Raki-inNo ratings yet
- Transport of Critically Ill Adults 2011Document1 pageTransport of Critically Ill Adults 2011velocity25No ratings yet
- Drug Classificati On Indications Action Route/Dos e Side Effects Patient Teaching Nursing ImplicationsDocument7 pagesDrug Classificati On Indications Action Route/Dos e Side Effects Patient Teaching Nursing ImplicationsJenny NguyenNo ratings yet
- Administering Vaccines To AdultsDocument1 pageAdministering Vaccines To AdultsPaul Anthony LoricaNo ratings yet
- Drugclasses Pharmacologypart 1 PDFDocument25 pagesDrugclasses Pharmacologypart 1 PDFSutanya100% (2)
- Drugs for Respiratory DisordersDocument1 pageDrugs for Respiratory DisordersEman ShalabyNo ratings yet
- Ed Adult and PaedsDocument2 pagesEd Adult and PaedsPrashin RocharamNo ratings yet
- Common Prefixes and SuffixesDocument5 pagesCommon Prefixes and Suffixestriddle1969100% (1)
- Fluid Overload Student PagesDocument4 pagesFluid Overload Student PagesJess OswaldNo ratings yet
- Drug Classes and Brand NamesDocument6 pagesDrug Classes and Brand Namesremyde07No ratings yet
- Sign of Diseases PDFDocument5 pagesSign of Diseases PDFJagveer Chauhan100% (1)
- Parenting Styles: - Dictatorial or AuthoritarianDocument45 pagesParenting Styles: - Dictatorial or AuthoritarianCourseTree LearningNo ratings yet
- PG PREPARATION - Mnemonics in PharmacologyDocument12 pagesPG PREPARATION - Mnemonics in PharmacologyRaveen KumarNo ratings yet
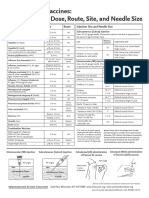
- Administering Vaccines: Dose, Route, Site and Needle Size GuideDocument1 pageAdministering Vaccines: Dose, Route, Site and Needle Size GuideKate Lucernas MayugaNo ratings yet
- Semester 2 Drug ListDocument7 pagesSemester 2 Drug ListNam_Pham_6481No ratings yet
- Drug CardsDocument3 pagesDrug CardsDave HillNo ratings yet
- NOAC ChartDocument2 pagesNOAC Chartsgod34No ratings yet
- Dka Guidelines - 2012Document4 pagesDka Guidelines - 2012djizhieeNo ratings yet
- Pharmacology Main DrugsDocument14 pagesPharmacology Main DrugsSabir KhanNo ratings yet
- Drug CardDocument1 pageDrug CardPaul AlfonsoNo ratings yet
- Hierarchy of O2 Delivery SystemsDocument1 pageHierarchy of O2 Delivery SystemsRevNo ratings yet
- Bam Slam Drug CardDocument4 pagesBam Slam Drug CardLeticia GonzalezNo ratings yet
- An Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFDocument6 pagesAn Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFkatherine dayagNo ratings yet
- Anti Microbial NotesDocument10 pagesAnti Microbial NotesMohammed Faisal UddinNo ratings yet
- Nephrotic and NephriticDocument27 pagesNephrotic and Nephritictam meiNo ratings yet
- @ Shopwithkey On Etsy Perfusion Drug Classification ChartDocument8 pages@ Shopwithkey On Etsy Perfusion Drug Classification ChartSutanyaNo ratings yet
- WWW - Qworld.co - in A-Z Disease List For NEETPG: IF Vit B Megaloblastic Anemia)Document5 pagesWWW - Qworld.co - in A-Z Disease List For NEETPG: IF Vit B Megaloblastic Anemia)Qworld100% (1)
- Drug Card Solu-MEDROLDocument2 pagesDrug Card Solu-MEDROLBenNo ratings yet
- OS217 LEC06 Rational Antibiotic UseDocument6 pagesOS217 LEC06 Rational Antibiotic Usegenerics54321No ratings yet
- Burn Stabilization ProtocolDocument2 pagesBurn Stabilization ProtocolAli AftabNo ratings yet
- AriaDocument57 pagesAriamushroom bestNo ratings yet
- Function of G I System: The Primary Digestive Functions Are Break Down Food Particles "Document113 pagesFunction of G I System: The Primary Digestive Functions Are Break Down Food Particles "cherryann_12100% (1)
- U World Endocrine FinalDocument12 pagesU World Endocrine Finalsean blazeNo ratings yet
- Combined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDDocument1 pageCombined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDnkuligowskiNo ratings yet
- Drug of Abuse (Table) PDFDocument2 pagesDrug of Abuse (Table) PDFtchanochNo ratings yet
- Examination of The Central Nervous SystemDocument3 pagesExamination of The Central Nervous Systemkenners100% (13)
- Labs Electrolyte ChartDocument1 pageLabs Electrolyte ChartmdcmepNo ratings yet
- 2020 Apr Common Treatment OrdersDocument32 pages2020 Apr Common Treatment OrdersAlistair LauNo ratings yet
- 10 Ecg Heart Rhythms PDFDocument1 page10 Ecg Heart Rhythms PDFMaybelline HiewNo ratings yet
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56No ratings yet
- Pharm Drugs ListDocument14 pagesPharm Drugs ListHumbe Oshun100% (1)
- Hopkins History Taking ArtDocument5 pagesHopkins History Taking ArtAnastasia TjanNo ratings yet
- History and Physical Exam SkillsDocument7 pagesHistory and Physical Exam SkillsAnonymous Sfcml4GvZNo ratings yet
- Heart Failure: Signs, Causes, TreatmentsDocument1 pageHeart Failure: Signs, Causes, TreatmentsTrisha VergaraNo ratings yet
- CPRDocument1 pageCPRjanet roosevelt100% (1)
- Heart Rhythms S SDocument3 pagesHeart Rhythms S SGloryJane100% (1)
- 2 0CommDiseaseIMPTVisionDocument3 pages2 0CommDiseaseIMPTVisionAndrea Patricia DaquialNo ratings yet
- Pharmocology Drug Cards: InnovarDocument33 pagesPharmocology Drug Cards: InnovarfaizaNo ratings yet
- Physical Examinations Respiratory System: InspectionDocument5 pagesPhysical Examinations Respiratory System: InspectionAzizan HannyNo ratings yet
- Medication List and InformationDocument9 pagesMedication List and InformationHealthAndFitnessGuyNo ratings yet
- Pharma GI CardsDocument16 pagesPharma GI CardsDoctorsHangout.comNo ratings yet
- Lung SoundsDocument6 pagesLung SoundsAira KieNo ratings yet
- Gastroesophageal Reflux Disease: What Is LES?Document3 pagesGastroesophageal Reflux Disease: What Is LES?Irish Eunice Felix100% (1)
- Common Signs and SymptomsDocument36 pagesCommon Signs and SymptomsJamil AimanNo ratings yet
- Suffixes and PrefixesDocument2 pagesSuffixes and PrefixesNiksNo ratings yet
- Rovamycin 3868 DR 1256036243912Document6 pagesRovamycin 3868 DR 1256036243912Ahmed El AlfyNo ratings yet
- Neutropenic Fever Empiric TherapyDocument5 pagesNeutropenic Fever Empiric TherapyRominaPulvermüllerSalvatierraNo ratings yet
- Management of Adult Febrile Neutropenia: 15011500-10123 99 Street Edmonton, Alberta T5J 3H1Document4 pagesManagement of Adult Febrile Neutropenia: 15011500-10123 99 Street Edmonton, Alberta T5J 3H1Tio Prima SNo ratings yet
- Aged Care Brochure PDFDocument12 pagesAged Care Brochure PDFMuhammad ZubaidiNo ratings yet
- CAP CURB-65 GuidelinesDocument1 pageCAP CURB-65 GuidelinesAndy LoakNo ratings yet
- DVTDocument60 pagesDVTAndy LoakNo ratings yet
- Jadwal Case Jadwal CodDocument2 pagesJadwal Case Jadwal CodAndy LoakNo ratings yet
- 018 Vs 022Document3 pages018 Vs 022kkorina5100% (2)
- Case Study ExamDocument4 pagesCase Study ExamAhmed Ismail Eatmann100% (1)
- Remembering The Good Old Days: Dr. Naresh TrehanDocument1 pageRemembering The Good Old Days: Dr. Naresh TrehanLife WatchNo ratings yet
- A 8418271112999392759Document3 pagesA 8418271112999392759nikhil parasia0% (1)
- Fu-Chan WeiDocument2 pagesFu-Chan WeiRoberto AlvaradoNo ratings yet
- The Expanded Program On ImmunizationDocument26 pagesThe Expanded Program On ImmunizationJudee Marie MalubayNo ratings yet
- BPH Zinc GreenTea Papaya LeafDocument13 pagesBPH Zinc GreenTea Papaya Leafteddy_shashaNo ratings yet
- Notes Skin Eye Ears Infections MicrobioDocument18 pagesNotes Skin Eye Ears Infections MicrobioChristiel John MagtibayNo ratings yet
- Drug StudyDocument8 pagesDrug StudyBien EstrellaNo ratings yet
- Lippincott Williams & Wilkins Nursing Book Collection 2013: Publisher What's IncludedDocument8 pagesLippincott Williams & Wilkins Nursing Book Collection 2013: Publisher What's IncludedDasrizal0% (1)
- Halleigh Ficarro: EducationDocument2 pagesHalleigh Ficarro: Educationapi-508687358No ratings yet
- Cipp 2015 AbstractsDocument88 pagesCipp 2015 AbstractsBuyanaaRise100% (2)
- Infection Control: Dr.T.V.Rao MD Professor of MicrobiologyDocument41 pagesInfection Control: Dr.T.V.Rao MD Professor of Microbiologytummalapalli venkateswara rao100% (1)
- I. The Problem and Its Background Ii. Demand and Analysis Review of Related Literature and Case StudiesDocument3 pagesI. The Problem and Its Background Ii. Demand and Analysis Review of Related Literature and Case StudiesPaulyn Mae Dela CruzNo ratings yet
- Diseases of The MouthDocument4 pagesDiseases of The MouthAhmed Gh Al-zechrawiNo ratings yet
- Missouri Counties Sue Drug Companies Over Opioid CrisisDocument274 pagesMissouri Counties Sue Drug Companies Over Opioid CrisisSam ClancyNo ratings yet
- Extended and Expanded Roles of Nurses 4Document1 pageExtended and Expanded Roles of Nurses 4Sivaprasad SNo ratings yet
- Feline Panleukopenia VirusDocument9 pagesFeline Panleukopenia VirusridhanoidNo ratings yet
- Chapter 15 OCD and Related DisordersDocument4 pagesChapter 15 OCD and Related DisordersCatia FernandesNo ratings yet
- Pioglitazone Hydrochloride Monograph For Professionals - DrugsDocument13 pagesPioglitazone Hydrochloride Monograph For Professionals - DrugssilvanaanggraeniNo ratings yet
- Work Performance of Month April 22Document3 pagesWork Performance of Month April 22Hari KiranNo ratings yet
- Remote Source Data Verification - EbookDocument23 pagesRemote Source Data Verification - EbookMichael BonettNo ratings yet
- Gambaran Radiologi TuberkulosisDocument36 pagesGambaran Radiologi TuberkulosisNathania PutriNo ratings yet
- Chunta 2020Document3 pagesChunta 2020intan jamaliahNo ratings yet
- StreptokinaseDocument2 pagesStreptokinasePramod RawoolNo ratings yet
- Timing of Antimicrobial Prophylaxis and Infectious Complications in Pediatric Patients Undergoing AppendicectomyDocument3 pagesTiming of Antimicrobial Prophylaxis and Infectious Complications in Pediatric Patients Undergoing AppendicectomyJuan J. Acosta VelásquezNo ratings yet
- Covid 19 Open LetterDocument5 pagesCovid 19 Open LetterKOLD News 13No ratings yet
- Mycoplasma MBBS lectureDocument19 pagesMycoplasma MBBS lectureSajjal Ali50% (2)
- 4-File3-Document 0 Dossier Robert F.Kennedy JR Du 05-02-2020 V.finaleDocument6 pages4-File3-Document 0 Dossier Robert F.Kennedy JR Du 05-02-2020 V.finaleVINYO ADANDOGOUNo ratings yet
- Policy For Exemption From Assessment and Examination FinalDocument28 pagesPolicy For Exemption From Assessment and Examination FinalGloria JaisonNo ratings yet