Professional Documents
Culture Documents
CH 31
Uploaded by
nhieuntnOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
CH 31
Uploaded by
nhieuntnCopyright:
Available Formats
C H A P T E R zzzzzzzzzzzzzzzzzzzzzzzzzzz
31
Low Lumbar Fractures Low Lumbar Fractures
zzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzz
Alan M. Levine, M.D.
Treatment of injuries to the low lumbar spine requires consideration of a number of additional factors beyond those relevant to injuries of the thoracic and thoracolumbar spine. These factors are related to the anatomic complexity of the lower lumbar spine, as well as the lordotic sagittal alignment and increased normal mobility of the lumbosacral junction. During the 1970s and 1980s, the lack of satisfactory instrumentation and techniques for reduction and stabilization of injuries in the low lumbar spine while preserving motion and alignment frequently resulted in less than optimal treatment results and led most authors to espouse nonoperative techniques as a better alternative.26, 49 Occasional reports, however, suggested that an operative approach yielded better anatomic results and perhaps even better functional outcomes.84, 133 Even with the more widely accepted use of pedicle screw xation for the lumbar spine in the late 1980s and early 1990s combined with more effective methods of sacral xation, some early, poorly conceptualized operative approaches to fractures in this region also led to early failure.4, 5, 62, 129 Although anterior approaches to these fractures have been advocated, rigid xation to the sacrum from an anterior approach has been problematic and requires a combined approach if anterior decompression is used.119 This problem caused some surgeons to accept chronic pain and the failure to return to preinjury occupation as the norm in this very young group of patients. Additionally, the relatively high complication rate associated with operative treatment of low lumbar fractures132 has caused some to advocate nonoperative over operative treatment for these patients. A number of studies in the last 10 years have suggested that nonoperative treatment yields satisfactory results in this group of patients, all of whom are relatively young at the time of injury (average age in most series, 27 years). However, many problems still exist with regard to interpreting data on these fractures inasmuch as most series report short to intermediate follow-up (<4 years) in a group of predominantly young male patients (27 years old) more often than not employed in manual labor tasks.21, 46, 107 Additionally, these conclusions are based on analysis of retrospective series with many discrep944
ancies and inconsistencies, such as marked variation in the elements of nonoperative care. In some series, recumbency for up to 6 weeks is included as part of treatment,4, 5, 8, 21, 124, 132, 133 whereas in others, it is not used. The type and duration of immobilization have also varied. Finally, the severity of injury has likewise not been uniform in comparisons of types of treatment4, 5, 132 in that patients with less structural instability and those without neurologic decit are most commonly treated nonoperatively whereas those with gross instability and neural decit are treated with surgical decompression and stabilization. All these factors, in addition to studies suggesting comparable complication rates124 for the two types of treatment, make selection of optimal therapy for an individual patient difcult. In the lumbar spine, anatomic and motion considerations have made instrumentation more difcult than in other regions of the spine. Injuries to the lumbar spine and upper part of the sacrum disrupt the normal lordotic alignment of the spine, and restoration of that lordotic alignment is critical to overall vertebral mechanics and spinal alignment in the sagittal plane. Failure to maintain or restore normal sagittal alignment in the lower lumbar spine after either elective fusion or fracture has led to the occurrence of late symptoms and even degenerative changes in long-term follow-up. The lumbosacral junction in particular must resist a number of large forces, but it must also permit a signicant amount of motion. It has therefore been difcult to achieve anatomic reduction and reconstruction of the lumbar spine and sacrum until the most recent advances in instrumentation. This difculty has led many authors to suggest either limited procedures and goals or benign neglect as the method of treatment of low lumbar and sacral injuries. Fixation to the bone of the sacrum has been even more problematic. These numerous features and problems distinguish fractures of the lower lumbar spine from the more numerous and common fractures at the thoracolumbar junction. More accurate diagnostic imaging studies, as well as advances in instrumentation techniques, should now allow us to treat injuries of the lumbar spine with the same
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
945
degree of accuracy and competence as more proximal spinal injuries. To do so, however, we must have a clear understanding of the anatomic and functional differences that distinguish the lumbar spine from the remainder of the more proximal areas of the spine. As described in Chapter 30, a specic set of technical considerations and xation methods are applicable to the treatment of spinal trauma in the thoracic region (T2T10), and similarly, a set is applicable to the thoracolumbar junction (T10L1). Fractures of the second lumbar vertebra form a transitional group, both functionally and technically, between those of the thoracolumbar junction (T10L1) and those of the lumbar region (L3S1). The major differences in anatomic considerations and techniques apply predominantly to L3S1, whereas L2 should be considered the transitional level because treatment at this level involves borrowing techniques from above and below. The treatment goals for spine trauma in general are (1) anatomic reduction of the injury, (2) rigid xation of the fracture, and when necessary, (3) decompression of the neural elements. For treatment of low lumbar fractures, we must add the considerations of (4) maintenance of sagittal alignment, (5) conservation of motion segments, and (6) prevention of frequent complications (e.g., recurrence of kyphosis, loss of sacral xation, pseudarthrosis). As the characteristics of the lumbar spine are reviewed, it will become evident that techniques discussed previously for the treatment of cervical, thoracic, and thoracolumbar spine injuries are not applicable to the treatment of lumbar spine injuries.
1 2 3 4 5 6 7 1 2 3 4 5 6 7 8 Line of gravity 9 10 11 12 Print Graphic Fixed kyphosis Flexible lordosis
ANATOMIC FEATURES
Presentation 1 2 3
zzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzz The rst critical anatomic consideration is the sagittal alignment of the lumbar spine. Normal kyphosis of the thoracic spine falls within a range of 15 to 49,155 whereas normal lumbar lordosis is generally thought to be less than 60. This curvature is in part determined by the slope of the sacral base, which averages approximately 45 from the horizontal. This angle is critical in determining the amount of shear force139 to which the lumbosacral junction is subjected (Fig. 311). Anatomic differences in the structure of the lumbar vertebrae and sacrum inuence therapeutic decisions and affect the attachment of xation devices differently than for proximal levels in the thoracic and lumbar spine. With caudal descent in the lumbar spine, the overall dimensions of the canal enlarge and the area occupied by the neural elements decreases. The cord in the thoracic region measures approximately 86.5 mm2 and is housed within a canal that averages about 17.2 16.8 mm2. Thus, in the thoracic region, the cord occupies about 50% of the canal area. In the thoracolumbar region, the conus broadens, as does the canal. The spinal cord usually terminates at approximately L1. In the lumbar region, the canal is typically large (23.4 17.4 mm2).41, 123 Here, the roots of the cauda equina are the only contents. In the sacrum, however, the diameter of the canal again begins to narrow and atten. In addition, with the normal, slightly kyphotic angle at the midpoint of the sacrum
Flexible lordosis
Center of gravity Fixed kyphosis
Sacrum Coccyx
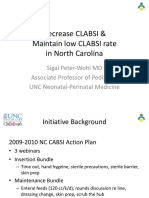
FIGURE 311. The spine is divided into four segments, two with relatively xed kyphosis (the sacral and thoracic spine) and two with relatively exible lordosis (the cervical and lumbar spine). The weight-bearing axis is anterior to the thoracic spine and thoracolumbar junction. Because it falls posterior to the vertebral bodies of the lumbar spine, the pattern of fracture with axial loading injuries is signicantly different in the lumbar spine than in the thoracic and thoracolumbar spine.
Copyright 2003 Elsevier Science (USA). All rights reserved.
946
SECTION II Spine
(S2S3), the roots are tethered in a relatively xed location. This anatomic arrangement allows less exibility in placing xation devices within the canal in the sacrum. In addition, the size and shape of the laminae change conguration at the various levels of the spine. The laminae in the thoracic and thoracolumbar region are rectangular, somewhat longer than wide. In the midlumbar spine, the width and length of the laminae equalize. At L5, the laminae are considerably wider than long (Fig. 312). The sacral laminae are extremely thin and might be absent in some areas. Similarly, it has been shown that in the lumbar spine, the minimal and maximal pedicle diameters increase to reach a mean minimal diameter of approximately 10 mm at L5 and 8.5 mm at L3.131 With the increasing emphasis on innovative methods of xation for injuries in the low lumbar spine,13, 92, 119 an understanding of the pertinent anatomic dimensions takes on new signicance. Previously, with hook xation or sublaminar wiring to the posterior elements, the only important consideration was posterior topographic anatomy. However, the dimensions, position, and orientation of the pedicles, as well as the shape of the vertebral body, are likewise critical. The initial anatomic description of pedicle morphology referable to pedicle screw xation was made by Saillant129 in 1976 and conrmed by two later studies from North America.77, 157 The critical features are sagittal and transverse width of the pedicles, pedicle length, pedicle angle, and chord length (depth to the anterior cortex along a xed orientation). These dimensions vary widely within regions of the spine (thoracic versus lumbar), but they also vary within the lumbar spine, with progression from L1 to L5. The mean transverse diameter measured on either computed tomography (CT) or an anatomic specimen was approximately 9 mm at L1 and increased to as much as 18 mm at L5 (Fig. 313). The sagittal width in the lumbar spine is relatively constant, with a mean of between 14 and 15 mm at all levels (see Fig. 313B). The angle of the pedicle axis generally increases in the lumbar spine, with a mean of about 11 at L1, 15 at L3, and over 20 at L5 (see Fig. 313A). Finally, the angle of insertion of the screw is critically important inasmuch as the shape of the lumbar vertebrae changes dramatically from L1 to L5 (see Fig. 313C and D). Because the distance between the pedicles is greater at L5 and the anteroposterior (AP) diameter of the vertebral body is effectively less at that location, the chord length or distance from the posterior cortex to the anterior cortex can vary dramatically with the angle of insertion. If screws are inserted perpendicular to the posterior cortex along a 0 axis, as originally described by Roy-Camille, the mean depth at L1 is about 45 mm, whereas at L5 it is only 35 mm. Increasing the angle of insertion to 10 or 15 or to the angle of the axis of the pedicle can increase the cortex-to-cortex distance by as much as 5 mm at L1 (to 50 mm) and 15 mm at L5 (to about 50 mm). For fractures of L5 or even very unstable shear injuries involving L4, xation to the sacrum is a necessary component. Understanding the three-dimensional anatomy of the various sacral levels, as well as the position of the neurovascular structures applied to the anterior surface of the sacrum, is critical for the conceptualization of
L2
Print Graphic
L3
Presentation
L4
L5
FIGURE 312. AD, The shape of the lumbar laminae and the relative size of the pedicles dramatically inuence the ability to position hardware. From L2 to L5, the length of the laminae becomes less and the width becomes greater. Therefore, hook placement is easier proximally in the spine but may cause impingement when placed over the lamina of L5 because of its relatively short length. However, pedicle xation is easier distally with the larger pedicle size.
adequate and safe xation to the sacrum. The anatomic structures that may be encountered at the level of the S1 body are the internal iliac vein, the lumbosacral plexus, and the sacroiliac joint. A safe zone bordered by the sacral promontory medially and the iliac vein laterally can,
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
947
however, be used for xation; it is about 2 cm wide and is invariably entered by orientation of a screw along the S1 pedicle.109 Screws placed laterally at either 30 or 45 are aimed at a smaller lateral safe zone. The more lateral orientation provides for a longer screw length of 44 mm.109 At the S2 level, the only vulnerable structure is the sigmoid colon on the left side. Penetration through the cortex by more than 1 cm is usually necessary for injury. At the S2 level, the thickness of the sacral bone is signicantly decreased from that of the S1 level, and thus, the holding power of the bone in an axis parallel to the placement of S1 would be signicantly less. To compensate for these deciencies, orientation of xation devices both proximally and laterally will signicantly increase the length of screw purchase and thus pull-out strength. Variations in the amount of cancellous and cortical bone mass in different regions of the sacrum signicantly affect xation possibilities and the risk of xation. Sacrum xation is more secure in the sacral ala because of its increased bone mass or in the sacral vertebral bodies, as opposed to xation in the very thin posterior laminar structures. Entry points for lateral and medial screw orientation at S1 are sufciently separate to make it
technically feasible to obtain both medial and lateral xation into S1, thus increasing stability and resistance to pull-out. The next signicant anatomic feature is the extreme exion-extension mobility of the lumbar spine in comparison with other areas. The thoracic spine is relatively stiff as a result of the orientation of the facet joints. Flexion-extension in the thoracic spine is limited, and in fact, rotation exceeds exion-extension at each level. At the thoracolumbar junction, exion-extension increases, whereas lateral bending and rotation decrease. The orientation of the facet joints in the lumbar spine becomes sagittal, and the facet joints become quite large.151 Therefore, the degree of freedom of motion progressively increases in exion-extension from L1 to L5 and decreases in rotation. Flexion-extension increases from approximately 12 at the L1L2 level to 20 at the L5S1 level, with lateral bending remaining similar at about 6.150 This extreme exion-extension mobility needs to be taken into account when considering injuries to the lumbar spine and sacrum because the relative position and orientation of one vertebra to another can change according to the position of the victim at
Pedicle axis
Transverse pedicle width
FIGURE 313. A, This axial view of a lumbar vertebral body shows the transverse pedicle width, which increases from L1 to L5. It also demonstrates the pedicle axis, which likewise increases from L1 to L5. B, A sagittal view of the vertebral body shows the sagittal pedicle width, which is relatively constant in the lumbar spine. C, This diagram shows an L1 axial view with the axis of the pedicle demonstrating the larger cortex-to-cortex distance. D, An axial view of L5 demonstrates how the anteroposterior length can increase with increasing angle.
A
Sagittal pedicle width
Print Graphic
Presentation
B
L1 vertebral body L5 vertebral body
00
Pedicle angle 100
00
Copyright 2003 Elsevier Science (USA). All rights reserved.
948
SECTION II Spine
impact. The extreme lumbar lordosis and lumbosacral angle can be attened dramatically by sitting and the spine oriented in a vertical rather than lordotic position. This change in angle and orientation contributes to differences in the relative incidence of specic types of injuries in the lumbar spine in comparison with those in more proximal regions.
Soft Tissue Injuries, Avulsion Fractures, and Ligamentous Injuries
Although this group of injuries may conceptually appear to be quite simple to understand and treat, it may be the most challenging because the injuries encompass a large and highly variable group. Until the early 1990s, these injuries were very poorly imaged because we relied on plain radiographic and CT scan ndings that were merely indirect evidence of the soft tissue and ligamentous injury. In some cases, these ndings poorly reect the force imparted to the spine or the subsequent severity of the injury. The improved use of magnetic resonance imaging (MRI) has at least allowed the physician to directly visualize the location of the injury; however, direct correlation between the visualized soft tissue or ligamentous injury and its effect on spinal stability has still not been claried. The signicant force needed to overcome the muscular and ligamentous restraints of the lumbar spine should be considered when evaluating these problems. For example, fractures of the transverse processes of the lumbar spine may represent several different injuries, depending on the mechanism. The signicance of an L5 transverse process fracture associated with a vertical shearing injury to the pelvis is different from that of multiple transverse process fractures. A more severe injury would normally be expected from a direct blow, such as when a pedestrian is struck by a motor vehicle, and a less severe injury from indirect muscular tension. The signicant force produced by the paraspinous musculature at the time of impact can result in an avulsion fracture of the transverse process (Fig. 314). More severe injuries can be accompanied by nerve root avulsion at the same level. Before any treatment and especially in combination with other signicant bony injuries, avulsion fractures should be thoroughly investigated to ascertain that the nerve root exiting at the level of the transverse process is intact. Preoperatively, myelography often does not demonstrate dye leakage at the level of the avulsion, but preoperative MRI or intraoperative exploration at the time of surgery for an associated injury might conrm the diagnosis (see Fig. 314). End-plate avulsion106 is a recognized phenomenon in adolescent patients. Disc herniation can occur in an adult who sustains signicant trauma, whereas in a child, the ligamentous attachments are somewhat stronger than the bony attachment of the end-plate (Fig. 315). Therefore, end-plate avulsion with displacement and neurologic ndings might be present. This pattern of injury can be visualized by a combination of CT and MRI and should be treated by excision of the end-plate fragment, which usually resolves the neurologic symptoms completely. End-plate avulsion is most frequently seen in adolescents and young adults at the L4L5 and L5S1 levels.42 In a younger child, it might occur only with avulsion of the cartilaginous ring apophysis. In adolescents and young adults, an isolated portion of the limbus or the entire bony end-plate can fracture off.42 Neural impingement is the result of both the bony fragment and disc herniation.42, 61, 145 Disruption of the posterior ligamentous complex (i.e.,
LUMBAR SPINE INJURY PATTERNS
zzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzz Most operatively treated fractures of the thoracic, thoracolumbar, and lumbar spine occur at the thoracolumbar junction. As a result of the anatomic differences previously discussed, the relative incidence of patterns of injuries is different in the lumbar spine than in the thoracic or thoracolumbar spine. The thoracic spine is additionally stabilized by the rib cage, whereas the thoracolumbar junction is a transitional zone at the end of a relatively stiffer segment. The lumbar spine is protected by only the abdominal and paraspinous musculature and is more subject to forces such as distraction and shear. In addition, factors extrinsic to the spine, such as the type of accident (motor vehicle accident versus fall) and the use of restraints such as lap belts versus shoulder harnesses, also inuence the number and types of injuries. For instance, the use of a lap belt alone by a passenger in a motor vehicle accident predisposes to exion-distraction injuries of the lumbar spine.7, 114 Because the lower lumbar spine and lumbosacral junction are normally quite lordotic, severe exion injuries are less common than in the thoracic or thoracolumbar spine. The extreme exion-extension range of motion frequently tends to negate the exion moment of an injury. Therefore, more low lumbar injuries are axial loading injuries as the spine is brought to a straight neutral position at the moment of impact and is then axially loaded. Some exion-distraction injuries occur as the pelvis or low lumbar spine becomes xed in a given position and the remainder of the body is exed and distracted over it. A variety of different injury patterns can occur in the lumbar spine. The purpose of dividing them into subgroups and classifying the injuries is to be able to predict their natural history and behavior. Easy recognition of these subgroups is important for determining optimal treatment. In addition, such classication should help the treating physician understand the nature of the instability16, 35 and thus construct a treatment regimen based on counteracting that instability. Although many classication systems exist, none has been totally successful in achieving those goals. Therefore, as in the other sections describing spinal injuries, these injuries are grouped and described by both radiologic criteria and their major deforming forces. The major forces contributing to the injuries are exion, extension, compression, lateral bending, rotation, distraction, and shear. Most injuries are caused not by a single force but by a major force with minor components from other, different types of forces.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
949
exion, which should lengthen the posterior ligamentous structures beyond their elastic limit. Supervised exion-extension radiographs after resolution of the initial spasm can make the diagnosis evident. Indications for surgical intervention and techniques are discussed in Chapter 27.
Wedge Compression Fractures
Wedge compression fractures (less than 50% anterior compression) result from a predominantly exion injury. They can vary from mild anterior compression with little or no instability to gross instability with signicant posterior ligamentous disruption. In all cases, the middle column is spared. By denition, the bony architecture of the posterior wall of the vertebral body must remain intact, and that is the critical dening difference between a compression fracture and a burst fracture. The degree of compression differs and results in the various fracture
Print Graphic
Presentation
FIGURE 314. Anteroposterior radiograph of the lumbar spine of a 24-year-old man involved in a motorcycle accident. The patient had a burst fracture of L1 and multiple avulsion fractures of the transverse processes at L1, L2, L3, and L4 (arrows).
supraspinous ligament, intraspinous ligament, facet capsules, ligamentum avum, and annulus of the disc) constitutes a continuum of injuries usually occurring in concert with other bony exion injuries.55, 58 If a signicant ligamentous injury occurs alone or in combination with a very innocent-appearing bony injury, such as insignicant anterior compression of the vertebral body (Fig. 316), it may be easily overlooked initially. If the patient has considerable spasm from the soft tissue injury, the full signicance of the ligamentous instability might be masked. CT scanning does not help demonstrate the extent of the ligamentous injury. Some evidence has indicated that MRI might be able to dene the degree of ligamentous destruction, but not the instability. Clinical correlation of these ndings is yet to be proved. Most of these patients do not have any neurologic decit.138 If a lap belt has been used without a shoulder harness, the patient might have signicant abdominal injuries. A high level of suspicion for lumbar ligament disruption should be present in any patient with L3, L4, or L5 anterior compression who has sustained a high-impact injury. To achieve compression of the anterior portions of the low lumbar vertebrae, the entire lumbar lordosis needs to be overcome and the patient placed in signicant
Print Graphic
Presentation
FIGURE 315. Lateral radiograph of the lumbar spine of a 16-year-old girl demonstrating an end-plate avulsion. She was involved in a motor vehicle accident and sustained complete paraplegia from the exion-distraction injury several levels above the area of bone injury. Note the avulsion of the end-plate of the vertebral body (arrows) with translation of the end-plate anteriorly, in addition to the exion and distraction of the posterior portion of the end-plate.
Copyright 2003 Elsevier Science (USA). All rights reserved.
950
SECTION II Spine
Print Graphic
Presentation
FIGURE 316. A 44-year-old woman was involved in a motor vehicle accident and sustained bilateral tibia fractures in addition to a fracture of L4. A, Lateral admission radiograph demonstrating alignment of her low lumbar spine at the time of acute evaluation. She underwent anterior compression (arrow) with satisfactory alignment in the sagittal plane. B, The anteroposterior radiograph does not show any apparent disruption of the posterior elements. She was therefore placed in an orthosis. C, Five months after the injury, the patient had signicant back pain after being out of the orthosis for 2 months. A lateral radiograph shows not only the anterior compression (arrow) but also disruption of the ligamentous restraints posteriorly with subluxation of the facets and apparent disruption of the interspinous ligament.
patterns. The exion load applied to the spine causes it to rotate about its axis of rotation and produces a fracture of the superior subchondral plate of the vertebral body (Fig. 317). Such fractures can occur at multiple adjacent levels in the lumbar spine. Care must be taken to differentiate this injury from one with a distractive force; in the latter case, severe ligamentous disruption can occur and the patient has signicant kyphosis and ligamentous instability. Compression fractures of the lumbar spine are a frequent consequence of severe osteopenia in older men and women. Although fractures of the lumbar spine occur less frequently than fractures of the thoracic region, once a single fracture has occurred, the risk of another fracture in either location is increased.115 Approximately 10% of white women older than 50 years have at least one fracture105; the proportion increases to almost 50% of women older than 80 years who have at least one fracture.100 These fractures may be associated with trivial trauma or may have no apparent trauma associated with them. They differ from compression fractures observed with trauma in younger individuals in that they may have a progressive course. When initially diagnosed at the time of onset of pain, these fractures may exhibit as little as 10% anterior compression with preservation of the posterior wall. However, over a period of 2 to 3 months, they can progress to almost 100% anterior compression with involvement of the posterior wall, canal compromise, and neurologic decit. Intervention by vertebroplasty may be appropriate in patients with increasing compression and persistent pain.
Burst Fractures
The fractures of most patients who ultimately require operative treatment of injuries to the low lumbar spine fall into this category. The injury patterns can differ markedly, depending on the level of the injury, as well as the predominant forces responsible for causing the injury. All burst fractures are produced by a combination of forces that always include exion and axial loading, with the pattern of the injury related to the relative proportions of the forces applied. These variations in pattern have been well described by Denis34 (see Chapter 30). In the upper portion of the lumbar spine (L2 and L3), either a predominant axial loading injury (Denis type A) or a predominant exion injury with some axial compression (Denis B) is possible. The former generally has little kyphosis but signicant axial compression of the body with comminution of both the superior and inferior end-plates. The body-pedicle junction is disrupted, and posterior element fractures also frequently occur. The latter consist of a fracture of the superior end-plate and a portion of the body, with retropulsion of bone into the canal. The critical features on CT are that the lower portion of the pedicle remains intact and in continuity with the body. The retropulsed fragment is the posterosuperior portion of the vertebral body. These injuries usually involve signicant anterior compression of the vertebral body, a variable amount of posterior ligament disruption, and sparing of the posterior elements (Fig. 318). A variant of this fracture type is the most common pattern that occurs in the low lumbar spine at the L4 and L5 levels. Fractures at L4 and
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
951
L5 demonstrate little kyphosis but can nevertheless cause signicant canal impingement. Reports by Levine and Edwards82, 84 indicate that most of these injuries occur in younger patients, with slightly more than 50% younger than 20 years.82, 84, 86 The fractures were equally divided between the L4 and the L5 levels and equally divided between patients with and those without neurologic decit. The mean canal compromise was only 47%, but in 5 of 22 patients, the retropulsed bone was so severe that it was in contact with the undersurface of the lamina. In 18 of 22 patients, the vertebral comminution involved approximately the upper half of the vertebral body, and the inferior halves of the pedicles were not comminuted and remained connected to the lower portion of the body (Fig. 319). The inferior section of the vertebral body was split into two halves in the sagittal plane, as described by Lindahl and coworkers.90 The mean loss of vertebral height was approximately 25% and was not as dramatic as in injuries to the thoracic and thoracolumbar spine. In addition, the measured kyphosis across the fracture level was only 8. This gure is less than the average traumatic kyphosis of approximately 21 at the thoracolumbar junction, but it
must be placed in context with the normal lordotic posture of the low lumbar spine. If a normal value of approximately 15 of lordosis is accepted for each level (L4L5 and L5S1), the total relative kyphosis is approximately 23 (although the absolute kyphosis is only 8). These gures are compatible with the amount of deformity seen in comparable injuries at other levels. A smaller number of patients with L4 and L5 fractures have a classic burst fracture pattern (Denis A) (Fig. 3110). This pattern also occurs more commonly in the upper portion of the lumbar spine at L2 and L3 and is characterized by marked widening of the pedicles on the AP radiograph, along with comminution of the pedicles and disruption of the body-pedicle junction. A large retropulsed fragment of bone and severe comminution of the anterior portion of the body are frequently seen. This scenario represents one extreme of the spectrum of exion-compression injuries, with the dominant force being axial loading. Such a force complex yields more impressive comminution of the vertebral body, with less kyphosis. If the force is applied asymmetrically or if the patient twists during impact, a rotational or lateral bending component of the injury can be involved and induce scoliosis or lateral wedging (Denis E) (Fig. 3111). More recent studies have emphasized an additional feature of these fractures that is clinically signicant. A small proportion of patients have a longitudinal laminar fracture that seems to be associated with traumatic dural lacerations.25, 36 In patients with lumbar burst fractures, a sagittal split can occur in the spinous process. This split should be differentiated from a fracture or comminution of the lamina. An incomplete sagittal split of the spinous process is frequently recognized on CT. When combined with a burst fracture and neurologic decit, a dural tear is usually indicated87 (Fig. 3112). Nerve roots can be outside the dural sac and might in fact be trapped in the split in the lamina. When evaluating these fractures, care should be taken to distinguish this feature so that appropriate surgical intervention can be undertaken.
Print Graphic
Flexion-Distraction Injuries
Presentation
FIGURE 317. Lateral radiograph of the lumbar spine demonstrating an L4 compression fracture sustained during a motor vehicle accident. Note the compression of the anterior portion of the vertebral body. However, the posterior wall of the L4 body importantly remains intact with its normal biconcave appearance. The interspinous distance is not widened, and overall alignment of the lumbar spine remains within physiologic norms.
Although most exion-distraction fractures occur in the upper lumbar spine, less than 10% of all major fractures of the lumbar spine result from exion-distraction forces. They are usually a result of the pelvis and lower part of the spine being anchored in a xed position (e.g., by an automobile lap belt).7 On impact, the upper portion of the spine accelerates and is thus distracted and exed away from the xed lower portion. Three major types of injuries occur. The rst is a completely bony injury (Chance fracture), the second is a completely ligamentous injury (facet dislocation), and the third is part ligamentous and part bony. The implications for stability and treatment differ tremendously. The Chance fracture, described by Chance in 1948,22 is a pure bony injury with a fracture line extending in a posterior-to-anterior direction through the spinous process, pedicles, and body. It is frequently associated with seat belt wear.60 The injury generally hinges off the
Copyright 2003 Elsevier Science (USA). All rights reserved.
952
SECTION II Spine
Print Graphic
Presentation
FIGURE 318. A 19-year-old man sustained a exion-compression variant of a burst fracture when thrown from a motorcycle. A, A lateral radiograph demonstrates kyphosis at the level of the fracture with compression of the anterior portion of the vertebral body. The posterior wall is likewise disrupted, but its height is diminished to a lesser extent. The posterosuperior corner of the vertebral body is retropulsed into the canal (arrow) and is causing signicant compression of the dural sac. Some widening of the interspinous distance has occurred, along with disruption of the interspinous ligament from the extent of exion. B, A computed tomography (CT) scan at the level of the injury demonstrates two important features. First, a large central fragment of bone has been retropulsed back into the canal and is causing high-grade neural compression. This fragment, at the level of the pedicles, is seen on the lateral view. Importantly, the pedicles are intact. No break is noted in the lateral wall of the pedicle, nor is the pedicle comminuted. The pedicle remains connected to the vertebral body, so any lordotic pressure applied to the pedicles will be translated to the vertebral body. The posterior neural arch is also intact, although it is not seen on this cut of the CT scan.
anterior longitudinal ligament. In its common form, it has no signicant shear component, nor is associated displacement present. It is infrequently associated with neurologic decit. The diagnosis can be made from lateral and AP radiographs. The lateral radiograph demonstrates a split in the spinous process, whereas the AP radiograph demonstrates a coronal split through the pedicles on both sides (Fig. 3113). Although a Chance fracture involves disruption of the posterior and anterior portions of the vertebral body, it is considered to be a stable injury and does not tend to angulate further into kyphosis. Two reviews of exion-distraction injuries55, 58 showed that this injury occurred only between T12 and L4, and that approximately 50% of the injuries were at L2, L3, or L4. This injury has an extremely high incidence of associated intra-abdominal injuries (50%), including bowel rupture and liver or spleen lacerations.* These injuries were originally classied by Gumley and associates,58 but the classication system was modied by Gertzbein and Court-Brown, who added anterior body
*See references 22, 31, 47, 53, 57, 60, 67, 70, 90, 99, 125127.
fractures.55 Although the system is somewhat complex, the principle of differentiating the ligamentous from the bony component of the injury is critical. Injuries with a fracture line traversing the spinous process, pedicles, and body are likely to achieve satisfactory union and stability if acceptable sagittal alignment can be maintained (see Fig. 3113). If the line of injury goes through the interspinous ligament and facets into the pedicle and body (Fig. 3114), satisfactory union of the body can occur, but residual instability can result from the posterior ligament disruption. Facet injuries of the lumbar spine occur infrequently. Levine and colleagues noted that bilateral facet dislocations below L1L2 represent only 10% of the total cases.85 The important feature of this type of exion-distraction injury is that it is mainly a soft tissue injury that results in complete disruption of the posterior ligamentous complex as well as the intravertebral disc. The bony architecture of the facets remains intact but totally dislocated. The minor compression of the anterior portion of the inferior body is merely a result of the severe ligamentous injury and does not contribute to the overall instability of the injury. The posterior walls of both vertebral bodies remain intact, and
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
953
Print Graphic
Presentation
FIGURE 319. The exion-compression variant (Denis type B) of a burst fracture is the most commonly seen pattern in L4 and L5 fractures. An 18-year-old man involved in a motor vehicle accident has rather typical ndings. A, A lateral radiograph of the metrizamide myelogram shows kyphosis of 8 across the L4 vertebral level. Minimal to moderate compression of the superior portion of the vertebral body can be noted. The degree of compression seen at this level is frequently less than that at more rostral levels. In spite of the minimal compression of the vertebra, a large retropulsed fragment can create signicant compression on the dural sac (arrow); the dural sac compression may be asymmetric, in which case it frequently traps a specic nerve root or roots and causes radicular symptoms. B, This patient had compression of his right-sided roots as a result of a retropulsed fragment (arrow) and a laminar fracture posteriorly on the same side with depression of the laminar fracture. The displaced posterior wall fragment and the depressed laminar fragment were in continuity on the right side and causing right-sided radicular symptoms. The pedicles remain intact in most patients with L4 and L5 burst fractures. The superior portion of the pedicle may be comminuted, but the lower portion remains attached to the vertebral body. C, In addition, the lower half of the vertebral body is most commonly split in half in the sagittal plane (arrows), with one pedicle remaining attached to each of the lower halves of the body.
Print Graphic
Presentation
FIGURE 3110. A smaller number of patients with L4 and L5 burst fractures have a classic burst pattern with comminution of the vertebral body and the pedicles. This 46-year-old man represents a typical example after a fall. A, A lateral radiograph demonstrates complete destruction of the L4 body with comminution of the pedicles and vertebral body. Little kyphosis is present, but there is a moderate degree of loss of height. The overall sagittal conguration of the spine remains relatively normal. B, An anteroposterior (AP) radiograph demonstrates splaying of the pedicles (arrows). Loss of height at the vertebral body can be noted on the AP radiograph as well. C, Computed tomography demonstrates severe comminution of the vertebral body with marked retropulsion of bone into the neural canal. There is a disruption of the body at the pedicle junction and, in fact, comminution of the pedicles. This patient has a sagittal split of the spinous process at L4 as well.
Copyright 2003 Elsevier Science (USA). All rights reserved.
954
SECTION II Spine
Print Graphic
Presentation
FIGURE 3111. A 17-year-old boy sustained a burst fracture of the L3 level with severe lateral compression. A, A lateral radiograph demonstrates loss of height of the disc space at L2L3 and slight kyphosis between L2 and L3. Comminution of the posterior elements (the spinous processes) is also noted. B, An anteroposterior radiograph demonstrates the major deformity: severe lateral wedging to the left side with severe compression of the left lateral side of the vertebral body. In addition, the transverse process and lamina of L3 on the right side are split (arrow).
canal compromise results from the translation of one intact vertebral ring in reference to the adjacent ring. This injury must be differentiated from a facet fracture, which is mechanically a different injury with comminution of the facets and sometimes also the laminae, pars interarticularis, and vertebral body. The severe translation seen in bilateral facet dislocations frequently results in signicant neurologic injury (80%)29, 54, 85 when the injury occurs at the thoracolumbar junction, but complete neurologic injury does not usually occur with these injuries in the low lumbar spine. Although severe translation resulting from disruption of the posterior ligaments occurs in association with severe disc disruption, the canal area is large enough that the nerve roots may be at least partially spared. Denis34 suggested that complete posterior disruption is insufcient to account for the degree of exion instability seen in this injury. Only incompetence of the posterior longitudinal ligament, anulus brosus, and disc could produce such a degree of translational instability. The anterior longitudinal ligament is often stripped from the anterior portion of the inferior body but remains intact. A number of authors66, 89, 101, 152 have suggested that this injury is a exion-distraction injury with the axis of rotation posterior to the anterior longitudinal ligament. Radiographs of bilateral facet dislocations are usually diagnostic.54, 85, 117 They demonstrate intact posterior walls of the vertebral bodies with signicant translation (36%) and lesser degrees of anterior compression and loss of disc height (Fig. 3115). AP radiographs of the lumbar spine often reveal the dislocation of the facets. CT scans conrm the pathology and demonstrate an empty facet sign,117 as well as the severity of canal compromise on sagittal reconstructions.54 The neurologic injury in patients with bilateral facet dislocations in the lumbar spine
is less severe than in those with dislocations in the thoracic and thoracolumbar spine, 80% of whom are complete paraplegics. This decreased severity is clearly a result of the larger canal area and the resilience of the cauda equina. Unilateral and bilateral facet dislocations and fractures at the lumbosacral junction may be associated with sacral fractures and are therefore addressed in the chapter on injuries to the sacrum (Chapter 35).
Shear Injuries and Mixed Instabilities
Only about 3% of all major lumbar spine injuries are complex combinations of deformities or signicant shear injuries. The addition of a shear force in combination with any other injury type markedly complicates the instability and treatment (Fig. 3116). For example, the combination of shear force with a bilateral facet fracture-dislocation or Chance fracture can cause complete rupture of the anterior longitudinal ligament and marked translation. Stiff spines, especially those affected by diffuse idiopathic skeletal hyperostosis or ankylosing spondylitis, are extremely susceptible to shear-type injuries, and dramatic deformity is noted on admission (Fig. 3117). Although not all shear injuries demonstrate tremendous deformity initially, a more subtle indicator of this extremely unstable injury is bidirectional translation (anterior as well as lateral) (Fig. 3118) on initial radiography. These injuries are most signicant in that they are grossly unstable and compromise the surgeons ability to achieve anatomically stable reduction. Recognition of disruption of the anterior longitudinal ligament and the circumferential nature of the injury is important. Most posterior xation techniques rely in part for their stability on an intact anterior longitudinal ligament. Care must be
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
955
taken to recognize this phenomenon and to be certain that the constructs used to reduce and stabilize the injury counteract the instability.
NEUROLOGIC DEFICIT
zzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzz The anatomic relationship of the conus and cauda equina to the lumbar spine largely determines the pattern of
Print Graphic
Presentation
neurologic decit. At the upper end of the lumbar spine, the conus broadens and can occupy as much as 50% of the canal diameter.123 In the distal portion of the canal, however, the cauda equina occupies less than a third of the cross-sectional area. Generally, spinal trauma from L2 down results in cauda equina (root-type) injuries, and thus recovery is different from that of injuries in the proximal portion of the canal. The relative position of the nerve roots within the dural sac is also important. The most posterior roots are usually those that exit more distally, because the more proximal roots are already anterior and lateral and somewhat more tethered by the bony foramen. This relationship is especially important for fractures of the lamina of L4 or L5, where roots may become entrapped after a traumatic dural laceration. These roots are generally the distal sacral roots, so injury to them may be evident only as changes in perineal sensation or subtle changes in bowel or bladder function. Neurologic injuries related to lumbar spine injuries are usually of two types. The rst is a complete cauda equina syndrome, which is often seen in severe burst fractures with canal retropulsion and large amounts of bone within the neural canal. The second type of injury is an isolated root injury or combinations of root injuries. These injuries may be nonrecoverable root avulsions and can occur in combination with avulsion of the transverse processes. Lesser degrees of root injury occur with canal impingement. Isolated root injury is common and is caused by a retropulsed fragment of bone catching the exiting root between it and the undersurface of the lamina. Root decits are also frequent in patients with low lumbar fractures that have sagittal splits in the lamina associated with dural tears. Posterior dural tears allow herniation of the roots outside the dural sac or entrapment within the spinous process or laminar fracture.25, 36, 87 Canal narrowing by translational deformity, such as in bilateral facet dislocation, is less likely to cause severe neurologic decit in the low lumbar spine than at the thoracolumbar junction. Burst fractures of the lumbar spine are associated with neurologic decit in about 50% of patients.
MANAGEMENT Indications
zzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzz
FIGURE 3112. A 62-year-old man sustained a severe burst fracture of L3 with an incomplete neurologic decit from L3 distally. Computed tomography demonstrates a burst fracture of L3 with severe comminution of the vertebral body and pedicles. In addition, the spinous process of L3 is split in a sagittal plane within the spinous process (arrow). On dissection of the posterior of the spine, this sagittal split is not evident. However, the combination of a sagittal split with a burst fracture of the lower lumbar spine and neurologic decit is pathognomonic of a posterior dural tear. On exploration, the patient was found to have a 3-cm laceration of the posterior aspect of the dural sac with herniation of nerve roots through the sac and entrapment of the roots within the sagittal split of the spinous process.
Various systems have been devised in an attempt to classify spinal injuries according to both mechanism and degree of instability. In addition, a number of denitions have been proposedfor example, stable versus unstable. A generic denition of spinal stability includes fracture patterns that are not likely to change position with physiologic loads and will therefore not cause additional neurologic decit or increasing deformity. Although many systems have been proposed that are applicable to lumbar spine injuries, no pragmatic system has been devised that clearly groups the injuries so that treatment approaches can be differentiated. Most classications of thoracolumbar trauma have either an anatomic reference14, 65 or a mechanistic reference,44 but all clearly fail to achieve the desired goal of classifying injuries according to subsequent treatment categories.
Copyright 2003 Elsevier Science (USA). All rights reserved.
956
SECTION II Spine
Print Graphic
Presentation
FIGURE 3113. An 11-year-old boy was a passenger restrained by only a seat belt (without a shoulder harness) in a motor vehicle accident. He sustained a exion-distraction injury with paraplegia at the T12 level. A, A lateral radiograph demonstrates a Chance fracture with the fracture line proceeding through the pedicles and the vertebral body in a line between the arrows. B, An anteroposterior radiograph shows both the transverse processes and the pedicle to be split in a coronal plane as marked by the arrows. Because this injury is strictly a bony injury, adequate bone-bone contact can be maintained and healing achieved without ligamentous instability.
Therefore, other criteria must be used to aid in making decisions about the treatment of lumbar and sacral fractures. In general terms, the indications for surgery in patients with lumbar and sacral injuries are the following: (1) the presence of detectable motion at the fracture site that cannot be controlled by nonoperative methods (instability), (2) neurologic decit, and (3) severe disruption of axial or sagittal spinal alignment. In lumbar and sacral
fractures, the presence of neurologic decit can indicate gross instability. With a large canalneural element ratio, signicant translation or angulation must take place to have neural injury. This rule is not universal, however, because transverse process fractures and avulsions can have accompanying nerve root avulsions. Additionally, in children, neurologic injury can occur at a level above that of the actual bony injury because of the differential elasticity of the cord and spinal elements.
Print Graphic
Presentation
FIGURE 3114. A 26-year-old man who had a car fall on him off a jack stand and cause severe exion sustained a variant of a Chance fracture. A, On a lateral radiograph, kyphosis is centered at L1. The fracture line goes through the interspinous ligament and into the pedicle on one side and the pars on the other side and into the vertebral body. Both end-plates are intact, and the fracture line is seen in the vertebral body (dotted line). Note the widening of the pedicles (arrows). B, Widening of the interspinous ligament is evident (arrows) on an anteroposterior radiograph, and the fracture line is seen obliquely traversing the pedicle on one side and the pars on the other (dotted line). Because the interspinous ligament is disrupted, residual posterior ligamentous instability occurs after healing of the bone injury.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
957
FIGURE 3115. A patient sustained a bilateral facet dislocation at L4L5. A, He presented with severe back pain, diffuse weakness below L4, and severe kyphosis, as seen in this preoperative photograph. B, A lateral radiograph shows severe translation of L4 over L5 with maintenance of height of the vertebral bodies. No fractures of the posterior wall were evident, although slight comminution of the anterosuperior portion of L5 occurred. C, A computed tomographic (CT) scan shows an empty facet sign. In addition, the translational and slight rotational deformities are apparent on this cut of the CT scan.
Print Graphic
Presentation
INSTABILITY In lumbar fractures, certain patterns of injury can be dened as unstable, even in the absence of neurologic decit. Patients with severe disruption of the posterior ligamentous complex from a exion or exion-distraction injury are considered to have unstable injuries. Treatment is clearly indicated, and there is little controversy regarding the appropriate treatment. Most authors believe that nonoperative treatment of ligamentous injuries does not restore stability and prefer limited operative stabilization. Similarly, exion-distraction injuries, such as bilateral facet dislocations with complete disruption of the posterior ligamentous complex and the disc, are considered to have gross ligamentous instability that will result in continued loss of sagittal alignment. In addition, shear injuries with circumferential disruption are known to be grossly unstable and in fact require operative stabilization. Burst fractures present a much more complex problem because they represent a spectrum of injuries. Patients who are
neurologically intact with minimal deformity require less aggressive treatment than do those with more severe injuries. The problem is predicting behavior of the injury based on static radiographic studies. Burst injuries that demonstrate signicant canal compromise, disruption of the anterior and posterior portions of the vertebral body, and laminar fractures are commonly considered unstable and require aggressive treatment. Mixed instabilities with gross displacement and shear injuries demonstrate markedly unstable clinical behavior. NEUROLOGIC DEFICIT The second criterion that constitutes an indication for treatment is neurologic decit. The benets of operative treatment of spinal injury have stimulated considerable controversy with regard to neurologic recovery of cordlevel injuries,23, 24, 27, 62, 81, 111, 136 but it is generally agreed that surgery is needed in the lumbar spine for the
Copyright 2003 Elsevier Science (USA). All rights reserved.
958
SECTION II Spine
reason that most injuries involve the nerve roots.25, 68, 87 Because the canalneural element ratio is very large, a small degree of canal compromise (30%) in the absence of severe deformity (kyphosis) tends to not be signicant with regard to neural recovery. A larger degree of canal compromise (50%) accompanied by high-grade neurologic compromise (cauda equina syndrome) can often be treated successfully by direct neural decompression.84, 103 In addition, specic root involvement with localized compression of the root can be improved by direct exploration of the root and decompression. Finally, patients with sagittal spinous process fractures, neurologic decit, and dural tears with roots outside the dural sac also benet from direct decompression and dural repair.25, 36, 87 DISRUPTION OF AXIAL OR SAGITTAL SPINAL ALIGNMENT The next indication for treatment is severe sagittal- or coronal-plane deformity. Most fractures of the lumbar spine result in kyphotic deformities and may be accompanied by translational and rotational deformities. Because normal lumbar sagittal alignment (i.e., lordosis) is critical to establishment of the normal weight-bearing axis of the body and to optimal function of the paraspinous musculature, restoration of sagittal alignment to normal is a critical element of treatment. It may be an important parameter in obtaining long-term pain-free functional results. However, the validity of this statement has not been fully veried because most of these injuries occur in
relatively young individuals and the follow-up in most operative and nonoperative series is still relatively short.4, 5, 21, 46, 72, 74, 107, 142 Clinically stable fractures that do not have signicant associated kyphosis or scoliosis can be optimally treated with external immobilization. However, fractures that have signicant kyphosis or other deformities that cannot be reduced and maintained with external immobilization need operative intervention for reestablishment of normal spinal alignment. Less emphasis was previously given to operative intervention because of the lack of appropriate methods to restore spinal alignment in a predictable manner. In fact, the use of spinal instrumentation for fractures of the lumbar spine resulted not in restoration of spinal alignment but in iatrogenically induced at back and other signicant alignment deformities with secondary symptoms. If the aim of treatment is accurate restoration of alignment, the surgeon must be certain that the method selected can achieve that goal.
Treatment Options
A number of treatment measures can be used for the management of lumbar fractures, and, in general, consist of nonoperative and operative treatment. Nonoperative treatment may include varying combinations of immobilization by cast or orthosis, postural reduction, recumbency, or immediate mobilization. For low lumbar injury, as with thoracolumbar injury, treatment regimens have not been very consistent from series to series. Operative intervention can involve various procedures, including (1) reduction, stabilization, and fusion of spinal fractures from a posterior approach; (2) indirect or direct decompression of neural elements from a posterior or posterolateral (transpedicular) approach; and (3) decompression or reduction, stabilization, fusion, and xation from an anterior approach. NONOPERATIVE TREATMENT Nonoperative treatment can be used for both stable and unstable injuries in the lumbar region. It is most often indicated for minor fractures such as spinous process fractures, transverse process fractures, compression fractures with less than 50% anterior compression, and Chance fractures. In addition, some burst fractures21, 65 can be regarded as stable and therefore appropriate for nonoperative treatment. The trend in the last 5 to 10 years has been an overwhelming transition toward nonoperative treatment for burst fractures of the low lumbar spine. This shift in approach has been the result of a number of factors, such as the relatively high complication rate with operative treatment of these fractures, loss of correction after operative treatment, and nally, failure to demonstrate improved functional results in shortto intermediate-term follow-up with operative treatment. However, no randomized, prospective studies have directly compared the two approaches. Currently, therefore, a major consideration in making the decision should be the degree of disruption of the posterior wall of the vertebral body and the extent of disruption in sagittal and axial alignment. Optimal nonoperative treatment of lum-
Print Graphic
Presentation
FIGURE 3116. This lateral lumbar radiograph demonstrates a severe shear injury in a 26-year-old man ejected from a motor vehicle. The spinal column is totally disrupted, and a fracture line (arrow) is traversing obliquely in an anterosuperior-to-posteroinferior direction through the body of L4.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
959
Print Graphic
Presentation
FIGURE 3117. A 31-year-old man with a known history of ankylosing spondylitis fell from a roof, landed on the upper part of his back, and sustained this shear injury. A, The lateral radiograph is the most dramatic, with the fracture line going through the ankylosed spine at the level of L4. There was 50% translation but relatively minimal angulation. B, The anteroposterior (AP) view shows little or no angulation or translation in this plane. C, Most likely as a result of the uniplanar translation and the signicant comminution of the spinal canal without retropulsion seen on this computed tomographic reconstruction, the patient had minimal neural decit. Anatomic reduction was achieved with multiple points of xation on the two rigid segments, and reduction was maintained in both the lateral (D) and the AP (E) planes at 1-year follow-up.
bar burst fractures should involve prolonged bedrest (3 to 6 weeks) before mobilization in an appropriate orthotic device. Failure to provide sufcient protection from axial loading forces by the use of bedrest can result in further deformity. At present, patients without neural decit or with only minor isolated root decit are optimal candidates for nonoperative treatment. Those with more dense
neural decits or severe deformity are better treated operatively. Even advocates of postural reduction have indicated that certain fracture patterns, such as bilateral facet dislocations, are not amenable to postural reduction and must be treated surgically regardless of the patients neurologic status.66 Optimal orthotic use for most fractures of the low
Copyright 2003 Elsevier Science (USA). All rights reserved.
960
SECTION II Spine
lumbar spine requires immobilization of the pelvis by a single leg spica cast or a thoracolumbosacral orthosis to x the relationship of the low lumbar spine. Immobilization by standard lumbar orthoses could actually accentuate motion at L4L5 and L5S1.45, 116 For upper lumbar fractures, a molded total-contact orthosis provides optimal immobilization. Care should be taken to not use an orthosis with a thoracolumbar extension (e.g., a Jewett brace) in the lumbar spine because it might increase motion at the index level by rigidly immobilizing more proximal levels. Thus, pain and deformity might increase in the low lumbar spine. Some authors have advocated the use of nonoperative treatment for unstable injuries. Treatment consisted mainly
of using bedrest to reduce gross malalignment and allow the fracture to begin to consolidate in the supine position before mobilization. Although such management was once an accepted method of treatment,11, 48 the current demands to reduce the length and cost of hospitalization, combined with the effectiveness of operative methods, render nonoperative treatment less desirable for unstable fractures. OPERATIVE TREATMENT GOALS AND INSTRUMENTATION Once the decision has been made to consider surgery for a patient with a spinal injury, the goals must be clearly
Print Graphic
Presentation
FIGURE 3118. A 44-year-old man was sitting in the bleachers as a spectator at a sporting event when a runaway van plowed into the stands. He sustained this L4L5 shear injury with complete three-column disruption. A, The anteroposterior radiograph shows both angulation and translation, whereas the lateral lm (B) shows predominantly translation (arrows). C, An axial cut of a computed tomographic scan through the disc space gives the best visualization of the severity of the injury, which consists of total disruption of the entire spinal column. D, Reduction and stabilization were achieved through the use of segmental xation, including reapproximation of the fractured pedicles to the vertebral body with central screws.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
961
dened to aid in selecting the appropriate procedure to achieve optimal results. With specic reference to the lumbar spine, the goals of operative treatment are reviewed here, and the various surgical methods by which those goals can be achieved are discussed. Details of the operative methods for specic injuries and their treatment plans are described subsequently. The major goals in the treatment of lumbar spine injuries are anatomic reduction of the fracture, maintenance of correction, decompression of neural elements (when indicated), maintenance of sagittal alignment, minimization of xation length, and minimization of the complication rate. The time from injury must also be considered because the efcacy of various methods changes with the time course. The controversy concerning the relative benets and risks of operative versus nonoperative treatment of fractures of the lumber spine continues to rage. Since the early 1990s, with the advent of patient satisfaction scales, measurement of the outcome of treatment has become more objective and is now considered to be as important as objective neurologic and radiologic criteria. A major problem still exists when attempting to decide on the optimal treatment for lumbar burst fractures. The average age of patients sustaining these injuries is around 27 years, and many are employed in manual labor at the time of injury. Although short-term studies have suggested that the fractures heal relatively reliably, the long-term outcome has not been clearly delineated. If we are technically able to restore anatomic alignment of the spine, do these patients do better with less pain and return to previous employment in both short- and long-term evaluation? Part of the problem in decision making is that some surgical techniques were used that either did not restore or did not maintain anatomic alignment.4, 142 Thus, the appropriate comparison is restoration of alignment with nonoperative treatment. With relatively short follow-up (<4 years), the trends in current studies suggest that patients with neurologic decit appear to recover more quickly and more completely with surgical intervention.68, 107 Some authors believe that nonoperative treatment of low lumbar burst fractures will provide satisfactory short-term results, but when the data are critically analyzed, most patients have a signicant degree of residual back pain and disability, even in the short term.4, 5, 21, 46 More accurate reduction and longer-term follow-up will yield different conclusions. In a series of 30 patients with a range of follow-up of 5 to 11 years (mean, 8.2 years) and with anatomic restoration of alignment in most patients, the incidence of back pain was less than 20% and the norm was return to preinjury employment.88 Thus, the current trend is nonoperative treatment for patients who are neurologically intact and have minimal to moderate deformity. For those with signicant deformity, neurologic decit, or both, operative treatment should give better long-term results. Anatomic Reduction of the Fracture The rst goal of operative intervention is anatomic reduction of the fracture. A general principle of achieving anatomic reduction is that the deforming forces that caused the injury must be directly counteracted by the
instrumentation system used to achieve the reduction. In addition, in the lumbar spine, the deforming inuence of normal physiologic forces must also be counteracted, specically, the shear force acting at the lumbosacral junction. For the lumbar spine, selection of an instrumentation system should be determined by the ability of that system to achieve reduction of the deformity and by the relative length of the instrumentation required. If a shorter construct can achieve the same degree of reduction and rigid xation, it should be used preferentially to maintain as many mobile levels as possible in the lumbar spine. Flexion and axial loading contribute in varying degrees to most deformities in the lumbar spine, and counteracting these forces should be carefully considered. The xation procedure should have an element of distraction and lordosis to restore normal alignment. Experimental data have demonstrated that devices offering variable and independent application of distraction and lordosis are more able to achieve anatomic reduction.17, 158 Not all instrumentation systems can achieve optimal results in all portions of the spine. In the following sections, some general types of instrumentation and their feasibility for use with different types of injury in the lumbar spine are considered. Over the last decade, a rapid transition has occurred in the types of instrumentation used for both elective fusion and xation of fractures in the lumbar spine. Although Harrington distraction rods were initially used for stabilization of spinal fractures, even in the lumbar spine, they proved inadequate because of the loss of lumbar lordosis imparted by the distraction. They failed either by hook dislodgement or by creating a lumbar at back. Even the rod-sleeve method, which allowed anatomic reduction with distraction while maintaining some lordosis, had a higher complication rate when used in the lumbar spine.40 Contoured rod systems with segmental xation by either wires or hooks (e.g., Moe rods, Harri-Luque, Cotrel-Dubousset, Synthes, TSRH [Texas Scottish Rite Hospital]) allowed correction of deformity and restoration of sagittal alignment for many patients, but with the disadvantage of requiring a longer length of instrumentation. The advent of pedicle screw systems allowed reduction and xation of lumbar injuries while immobilizing fewer levels, thus more easily maintaining lordosis with less hardware dislodgement. Whereas the early systems such as the Olerud device and the Fixateur Interne were bulky and complicated, more current systems have technical advantages over the early pedicle screw systems. Although no appreciable improvement in outcome was noted in the treatment of thoracolumbar fractures,156 the differences are more pronounced in the low lumbar spine. In addition, most pedicle screw systems can achieve rigid xation and maintenance of sagittal contours. Additionally, the length of instrumentation does not need to be increased when removing portions of the posterior elements for repair of dural lacerations or for direct root decompression. Pedicle screw systems are of two basic types: platebased systems and rod-based systems. Most plate-based systems have no signicant capability of achieving reduction other than by postural reduction on the operating table.39, 93, 128, 141 Rod-based pedicle xation devices37, 76, 94, 95, 118 allow progressive reduction of de-
Copyright 2003 Elsevier Science (USA). All rights reserved.
962
SECTION II Spine
formities after screw xation, with maintenance of correction. Anterior Procedures. Anterior procedures for decompression, reduction of deformity, and stabilization have been used in the acute setting. In the absence of instrumentation, the long-term results of anterior correction of deformity with the use of a strut graft have been poor in terms of maintenance of anatomic alignment.103 A tricortical bone graft cannot provide progressive correction, but when augmented by the use of a plate, it may be a satisfactory alternative in certain L3 and L4 fractures. Fixation to the sacrum is not truly feasible from an anterior approach, and xation to L5 can even be difcult because of the relationship of the hardware to the iliac vessels. The ability to slightly compress and distract is now built into the slotted holes and instrumentation of several different plate designs.69 This addition is an improvement over previous plates that simply functioned as neutralization devices. These plate systems now allow decompression and reasonable stabilization to be accomplished from an anterior approach for upper lumbar spine fractures. For the correction of deformity from spinal fractures that are more than 6 weeks old, the mechanics of correction are different because secondary changes have occurred that complicate the fracture deformity. Primary healing of the cancellous fractures has begun, along with scarring of the soft tissues. At this stage, an anterior procedure for release of tissues becomes important in achieving and maintaining correction as the complexity and stiffness of the deformity increase. When reduction is attempted with posterior instrumentation alone more than 6 weeks after injury, it is difcult to overcome the kyphosis that has resulted from the shortening of anterior structures and the formation of anterior bony bridges. Some preliminary evidence is now available that anatomic reduction can be achieved and maintained from a posterior approach with appropriate application of forces if no synostosis has formed anteriorly. Total reduction from an anterior approach alone can be difcult in these late cases because posterior scarring or healing of posterior element fractures may have occurred. In addition, most anterior spinal devices lack sufcient lever arms and rigidity of xation points to be able to apply forces adequate for achieving total reduction. Maintenance of Correction The second goal of surgical treatment, maintenance of correction, is related to the rigidity of xation and to the ability of the selected instrumentation to counteract both the deforming forces and the normal physiologic forces of the lumbar spine. Long-term results with regard to the rigidity of xation have been poor for devices that do not counteract all the deforming forces, such as straight distraction rods and segmental spinal instrumentation. In addition, in the lumbar spine, where construct length is important, shorter constructs impart more load bearing to the hardware and may therefore have a higher failure rate. The concept of load sharing either with intact posterior elements or with supplemental anterior graft should be considered. Experimental data on short constructs for the lumbar spine often lead to the conclusion that restoration of the anterior column with a strut graft is important,39, 59, 75, 96, 137 although in practice, load sharing with
the intact posterior elements, if properly applied, seems to be sufcient. In addition, in areas of the spine where stability of the construct is compromised by inadequate terminal xation (e.g., the sacrum), maintenance of long-term anatomic restoration of alignment has been unsatisfactory. Posterior devices that achieve rigid xation and counteract deforming forces can produce satisfactory results with hook or pedicle screw xation. The use of anterior grafts as the sole stabilizer after anterior decompression and correction of deformity has had disappointing results. More rigid anterior devices have improved the outcome in maintaining satisfactory long-term results.97 The combination of anterior surgery to restore stability of the anterior column plus posterior pedicle screw xation can allow optimal stability, but it requires more extensive surgery with higher risk and is probably not indicated except when anterior decompression is necessary. Even when the anterior portion is performed thoracoscopically, the operative time and relative risks are still high.119 Decompression of Neural Elements The third goal, decompression of neural elements, is not always a critical one for surgical treatment of lumbar burst fractures. Although it was originally thought that a patient who was neurologically intact but had signicant canal compromise might benet from neural decompression, it has been shown that this assumption is false. Late spinal stenosis does not occur in either operated or nonoperated patients in whom reasonably normal anatomic reduction is achieved. It has been well demonstrated that resorption of residual bone within the canal predictably occurs both with and without surgery.19, 28, 32, 79, 136, 143 Thus, the sole indication for neural decompression is neural decit. Neural decompression can be achieved in several different ways, both directly and indirectly, and the most favorable method depends on the specic clinical situation. Laminectomy alone rarely plays a role in decompression of retropulsed bone that has been retropulsed against the anterior portion of the dural sac. It is effective in removing pressure from a posterior fragment of lamina driven into the canal or in decompression of an isolated root. Signicant experimental50, 63 and clinical evidence27, 38, 83, 135, 147, 154 has indicated that immediate indirect decompression by ligamentotaxis and complete correction of the deformity can provide adequate decompression of the neural elements. This technique has been shown to be most effective in the rst 48 hours after injury. Transpedicular decompression is a direct posterior technique,62, 146 but one with limited visibility of the anterior portion of the dural sac and with results that do not differ from those of indirect decompression. In the low lumbar spine and sacrum, however, indirect decompression is not as successful because the technique depends on distraction and tensioning of the posterior longitudinal ligament. It is therefore less effective in an area of extreme lordosis or kyphosis. Thus, at L4 and L5, direct decompression by laminectomy or laminotomy can be effective in revealing the area of compression and allowing decompression by removal of the bone fragments that are compressing the dural sac or nerve roots. This technique can be done because limited retraction of the dural sac to achieve exposure is possible at this level. It is recommended only for areas of the spine involving the cauda equina. Direct
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
963
decompression is most easily performed when the compression is one sided and bilateral exposure is not necessary. It is technically easier when carried out within the rst 2 weeks after injury because the fragments are more mobile and more easily removed. In the upper lumbar spine, a transpedicular posterolateral approach to direct decompression might be indicated. In this case, removal of a portion of the lamina and the pedicle exposes the dural sac adequately on one side and allows direct decompression. For patients who have had inadequate indirect decompression with posterior instrumentation or who are initially seen late (more than 2 weeks after injury) and require decompression of the dural sac, anterior corpectomy and direct decompression are the most effective procedures. Some authors have advocated direct anterior decompression and stabilization in the immediate acute setting for the treatment of lumbar trauma, but the increased morbidity and potential for decreased stabilization noted with the anterior approach make it a somewhat less attractive alternative. In addition, the use of pedicle xation for the stabilization of especially low lumbar fractures allows laminectomy and posterior decompression along with a very short construct length, without compromising the quality of the reduction and stabilization. Maintenance of Sagittal Alignment The next important goal in the treatment of low lumbar fractures is maintenance of sagittal alignment. Any instrumentation system used for these fractures should be able to impart and maintain the lordosis of the lumbar spine and lumbosacral junction. When crossing the lumbosacral junction, as is the case with many low lumbar fractures, xation to the pelvis needs to be accomplished to maintain lordosis. Hook xation to the sacrum is inadequate.13 Several systems have used rods driven into either the sacral ala or the ilium; the latter has the disadvantage of crossing the sacroiliac joint. Most xation constructs crossing the lumbosacral junction require screw xation. Such xation is especially critical in maintaining the lumbosacral angle, lumbosacral lordosis, and overall sagittal alignment of the spine. Minimization of Fixation Length Minimizing xation length to maintain the maximal number of mobile lumbar segments is the next important treatment goal and consideration in instrumentation of fractures of the lumbar spine. However, satisfactory balance must be maintained between the number of levels requiring instrumentation to achieve satisfactory reduction plus stabilization and preservation of important lumbar motion segments. Fixation rigidity should not be compromised to shorten levels, such as with the use of Luque rectangles in fractures of the lumbar spine. Similarly, plate xation requires an adequate number of screws above and below the fracture. Even the Cotrel-Dubousset system has been found to be inadequate in maintaining alignment with the use of short constructs1, 9, 10 (less than four levels) and requires augmentation with an anterior strut graft to achieve anatomic reduction. Parker and colleagues122 attempted to quantify the degree of disruption of the anterior column to understand which fractures had
sufcient residual integrity to allow short-segment posterior instrumentation. Although this concept is helpful, in reality, the most stable fracture patterns that would maintain alignment with short-segment xation would also most probably maintain alignment with nonoperative treatment. Even anteriorly, attempts have been made to shorten the construct to only the injured segment.110 Thus, when selecting a construct, the surgeon should keep in mind both the rigidity of xation and the length of the construct to avoid compromising other treatment goals. Minimization of the Complication Rate The nal treatment goal of lumbar and sacral fractures is to minimize the extremely high complication rate associated with instrumentation of these injuries. The major complications are pseudarthrosis, failure of sacral xation, and iatrogenic at back.80 Care must be taken when achieving the other treatment goals so that the instrumentation system does not jeopardize the results with an unacceptably high complication rate.
Standard Techniques for Specic Types of Injuries
MINOR BONY, DISCAL, AND LIGAMENTOUS INJURIES Most minor bony injuries, such as avulsion fractures, spinous process fractures, and ligamentous strains, are satisfactorily treated by external immobilization for symptomatic relief. Patients with posterior ligamentous instability but no signicant fracture might not be initially recognized, but once the spasm of the acute injury has subsided, exion-extension radiographs can usually demonstrate the instability. With a minor degree of disruption (sprain), external immobilization for 6 weeks to 2 months can allow sufcient healing to achieve symptomatic relief and stability. If the disruption is complete, with tearing of the ligamentum avum and annulus and anterior wedging of the disc space on exion-extension radiographs, arthrodesis may be necessary to restore sagittal alignment and control the ligamentous instability (Fig. 3119). Avulsion fractures of the transverse processes can be treated symptomatically by external immobilization to support the severe muscular trauma associated with the more minor bony injury. Transverse process fractures associated with more severe bony injury can be secondarily treated by immobilization of the primary injury. End-plate avulsions in children simulating disc herniation in the acute injury setting require surgical intervention for direct decompression after appropriate diagnostic studies.40, 42, 145 A laminotomy, as used for discectomy, is generally sufcient to allow excision of the protruding portion of the end-plate. The remaining portion of the end-plate generally heals without further intervention. ANTERIOR WEDGE COMPRESSION FRACTURES Compression fractures of the lumbar spine are relatively frequent as either single or multiple injuries. Their outcome is usually favorable, except in an osteopenic
Copyright 2003 Elsevier Science (USA). All rights reserved.
964
SECTION II Spine
Print Graphic
Presentation
FIGURE 3119. A 44-year-old woman whose initial radiographs are shown in Figure 316 presented 5 months after injury with severe kyphosis and ligamentous instability. A, Unfortunately, her maximal hyperextension radiograph shows only minimal correction of kyphosis (arrow). The patient underwent posterior correction, stabilization, and fusion of her kyphosis. B, She eventually achieved solid arthrodesis and is pain free with no evidence of instability.
patient. The two most common diagnostic problems are failure to recognize accompanying severe ligamentous disruption and the incorrect identication of a burst fracture as merely a compression fracture. In evaluating these injuries, care must be taken to prove that the posterior wall of the vertebral body remains intact. Another common pitfall in the treatment of these injuries is failure to recognize the extent of the injury. Although the degree of sagittal-plane deformity might not be severe, CT scanning is indicated to conrm the integrity of the posterior wall of the vertebral body. Careful examination of centered AP and lateral plain radiographs will differentiate the two injuries in most cases. Often, the lateral radiograph shows displacement of the posterosuperior corner (Fig. 3120). Comminution of the posterior wall converts the injury to the more signicant burst pattern, which alters the prognosis and the treatment program. In addition, the surgeon must be certain that the compression fracture is not accompanied by ligament disruption (see Fig. 3119). For wedge compression fractures with loss of less than 50% of the height of the vertebral body, no ligamentous instability generally exists. The goal of treatment is to prevent further anterior compression and residual kyphosis.78 Nonoperative treatment, even in hyperextension, cannot restore vertebral height, but affected patients are still best treated nonoperatively. Careful attention needs to be paid to the ability of the orthosis chosen to immobilize that segment of the spine. Compression fractures of L2L4 are not hyperextended by a Jewett brace and might in fact be made worse. These fractures require a lumbar orthosis, such as a chair-back orthosis, Norton-Brown brace, or total-contact orthosis. Compression fractures of L5 are not well immobilized by the standard lumbar orthoses, and in fact, motion at the L5 level is accentuated by the use of a lumbar orthosis, which blocks movement at the other levels.45, 116 Immobilization of L5 fractures requires a
single leg included in the orthosis to immobilize the lumbosacral junction. Immobilization needs to be extended for a period of 3 months, until the vertebral body has consolidated. After immobilization, the patient should be checked with exion-extension radiographs to determine whether any residual instability is present. Increasing compression during the course of treatment that interferes with the normal lordotic sagittal alignment of the spine might require a change in treatment, surgical restoration of alignment, and single-level arthrodesis. Compression fractures secondary to osteoporosis require two critical elements in their treatment. First, compression fractures in the lumbar spine can result in a signicant retroperitoneal hematoma, which in an elderly patient may result in an ileus. Additionally, establishment of a pain medication level that is tolerated by an elderly patient may be difcult. Therefore, it is recommended that the patient be admitted to the hospital for a period of 24 hours after the diagnosis is made to ascertain that an ileus that could potentially result in life-threatening dehydration does not develop. Second, the pain medication needs to be regulated so that the patient is functional but sufciently comfortable. Next, if the patient is not already taking a bisphosphonate, a basic workup should be done to establish the level of osteopenia, and a treatment program should be initiated. Finally, immobilization should be applied to help relieve the pain. A semirigid corset is sufcient for lumbar fractures, and it is usually well tolerated and helps relieve pain. After discharge, follow-up should be scheduled in 1 week for repeat radiographs and to ascertain that the pain relief is acceptable. Follow-up should again be performed at 1 month for careful evaluation of healing of the fracture and for measurement to determine whether the vertebral body is continuing to collapse. If severe pain and continued collapse are still present at 4 weeks, consideration of vertebroplasty or kyphoplasty should be made at that time.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
965
BURST FRACTURES OF THE LUMBAR SPINE Most patients who sustain injuries to the lumbar spine that require operative stabilization have burst fractures. The key to selecting the most appropriate treatment for these patients is recognition of the components of the fracture pattern. As previously described, all burst injuries involve comminution of the anterior portion of the body and signicant involvement of the posterior wall (middle column), along with retropulsion of bone into the canal. The types of burst fractures that occur most commonly in the lumbar spine are Denis A (comminution of the entire body and the body-pedicle junction with or without involvement of the posterior elements) and Denis B (comminution of only the upper end-plate with an intact body-pedicle junction and usually sparing of the posterior elements). These two fracture types have reasonably equal distribution at L2 and L3, but the Denis B fracture predominates at L4 and L5. Lateral burst fractures (Denis E) are also occasionally seen. Review of the care of these injuries illustrates most of the techniques required for the surgical treatment of lumbar injuries. Differentiation between the types of treatment appropriate for fractures occurring in the upper and the lower lumbar spine is necessary for optimal results. However, with the adoption of pedicle screw xation as the standard for the lumbar spine, constructs used in the upper and lower lumbar spine are not dissimilar, with the exception of length. Flexion-compression (Denis B) injuries, a subset of burst fractures, are characterized by fracture of the posterior wall of the vertebral body with retropulsion of the posterosuperior corner into the spinal canal causing compression. The critical feature on AP radiographs and CT scans is that the pedicles are not splayed. On CT scans, it is evident that they are still attached to the lateral sides of the vertebral body, although a large central fragment is present and can cause canal compression. This nding is usually accompanied by a signicant degree of kyphosis. The instrumentation construct used for this area needs to
be able to correct the kyphosis in the upper lumbar spine and restore lordosis in the lower lumbar spine. This ability is related to the length of xation and thus the length of the lever arm applying the forces, as well as the rigidity of the system and the types of forces applied to the screws.121 Previously, hook and rod constructs such as the Edwards rod-sleeve method or multiple-hook systems such as the TSRH, Cotrel-Dubousset, and Isola were appropriate for the treatment of upper lumbar fractures because the length of the instrumentation was not thought to be as critical in this region. However, certain systems were associated with a signicant rate of loss of correction, nonunion, and hook dislodgment, especially related to the upper level, and all were dependent on intact posterior elements. With more common use, pedicle xation constructs have slowly replaced most of these other systems in the lumbar spine, and they clearly maintain their effectiveness and use for thoracolumbar and thoracic fractures. The application of these systems has been thoroughly discussed in Chapter 30. Before discussing the use of surgical techniques for lumbar fractures, it must be reemphasized that the role of surgical treatment of these injuries is still being dened. The most common current surgical indications are traumatic dural lacerations, neurologic decit (other than isolated root decit), and signicant deformity (greater than 25 of relative kyphosis with or without decit). Although most of the reports to date have relatively short (<5 years) follow-up,4, 5, 107 data on intermediate-length (5 to 10 years) follow-up are now becoming available.132 Pedicle screw xation for upper lumbar injuries can be used over more levels to achieve rigid xation, especially for fractures with more disruption of the anterior column. Thus, for an L2 fracture, the type of construct applied can vary considerably. If it is a Denis B fracture, it may require only one screw above and below (L1 and L3) (Fig. 3121A), or it may also accommodate a screw directed into the lower portion of the fractured body for a three-screw construct (two screws above and one below
FIGURE 3120. A, An L4 burst fracture might be mistaken for a simple compression fracture of L4 on this lateral radiograph. The key to the diagnosis is the posterosuperior corner (arrow) of the affected vertebral body (L4). B, The posterosuperior corner is retropulsed into the canal as conrmed on computed tomographic (CT) scans. Although the comminution of the vertebral body and the loss of height are unimpressive, the degree of canal occlusion and the overall structural disruption of the vertebral body are not fully appreciated except on the CT scan.
Print Graphic
Presentation
Copyright 2003 Elsevier Science (USA). All rights reserved.
966
SECTION II Spine
Print Graphic
Presentation
FIGURE 3121. A, The use of pedicle screw constructs or hybrid screw-hook constructs allows correction of both the exion component and the compression component of a deformity. A number of options exist, and the length of the construct and the number of screws used depend on the stability of the fracture, as well as the level of the fracture. For relatively stable Denis B burst fractures, one screw above and below the fractured level is adequate at the L2 or L3 level. B, For Denis B fractures requiring a longer lever arm for reduction or those that are less stable (more disruption of the anterior column), two screws above and one below can be used. C, For Denis A fractures with severe comminution, two screws above and two below increase the stability of the construct and also increase the lever arms to achieve reduction. D, Alternatively, some authors suggest an anterior graft to restore the stability of the anterior column; however, this procedure increases the duration of surgery and risk and is harder to justify unless the patient requires anterior decompression for a neurologic decit.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
967
Print Graphic
Presentation
E
FIGURE 3121 Continued. E, In certain fractures increased stability can be achieved by angling a screw into the noncomminuted portion of the fractured vertebral body.
the fracture) to achieve greater reduction force (Figs. 3121B and E and 3122). For Denis A fractures (Fig. 3123) with complete anterior disruption, the same two screws above (T12 and L1) and either one below (L2) or two below (L2 and L3) can be used (see Fig. 3121B and C). Some authors advocate restoration of the anterior column with a cage or graft and an adjunctive one above and one below the posterior construct (see Fig. 3121D). For fractures of the upper lumbar spine, the length of xation is not as critical in terms of incorporating distal segments and maintaining motion. Stability and maintenance of correction are important. For the lower lumbar spine, the length of xation becomes more critical. Pedicle xation has the advantage of allowing xation across short levels (three segments, two interspaces). For an L4 burst fracture, instrumentation extends from L3 to L5 (see Fig. 3121E), and for an L5 burst fracture, instrumentation extends from L4 to S1. Various pedicle xation systems that can achieve these goals are currently available.* Technically, the existing xation systems have three
*See references 12, 18, 26, 38, 39, 43, 56, 91, 98, 104, 130, 134, 143, 153.
major differences. The rst involves the number of points of xation on the spinal column. Most spinal xators allow only two points of xation, generally above and below the fracture site (Fig. 3124A). Most plate systems (Steffe, Roy-Camille) and rod-screw systems (Cotrel-Dubousset, TSRH, Synthes, Modular) have xation at each instrumented level (at least three points), including the apical or fractured level (Fig. 3124B). Second, the direction of sacral xation is down the pedicle of S1 into the body (see Fig. 3124C) or laterally into the sacral ala (see Fig. 3124D). Bidirectional or two-point xation into the sacrum can be achieved with some systems to enhance the xation of L5 fractures. Third, pedicle screw systems can be static and simply become rigidly xed in the position attained by postural reduction (plate system), or they can allow progressive reduction of the fracture after the insertion of screw xation and attachment of the device by the application of progressive force. The following discussion of pedicle xation illustrates the basic principles of the technique. Initial evaluation with appropriate AP and lateral plain radiographs and CT scans to determine pedicle and vertebral size and location is critical. Patients are positioned on a standard operating room table in a neutral position on longitudinal rolls or a radiolucent spinal frame. A radiolucent operating table allows for easier radiographic control of screw placement. In either case, AP and lateral imaging or radiographic control for positioning of the pedicle screws is mandatory. A midline posterior incision is used. Dissection is done carefully with a cautery to avoid excess motion of the injured spine. Frequently, spinous process and posterior element fractures are encountered when exposing L4 and L5 fractures. If the spinous processes and the interspinous ligament are intact, the ligament should not be removed but instead preserved during the dissection. The integrity of the interspinous ligament should be maintained at the levels just proximal and distal to the construct to prevent hypermobility postoperatively. The ligament can also be used during closure to restore the integrity of the lumbodorsal fascia. Care is also taken while stripping soft tissue from the spine at the proximal level that the capsule of the adjacent facet joint that remains unfused not be disturbed when exposing the transverse process (see Fig. 3125A). Specically, the L2L3 facet joint (adjacent to the L3 transverse process) for an L4 burst fracture and the L3L4 facet joint for an L5 burst fracture should remain unfused, and their capsules must be competent to resist the increased stress on adjacent instrumented levels. The pedicle screw can be placed inferior and lateral to that facet joint so that it does not impinge on the unfused facet and cause secondary changes. Exposure of the transverse processes of the appropriate levels can reveal fractures and landmarks helpful in screw placement. The facet capsules are removed only at the two or more levels to be fused. When fusion is extended to the sacrum, the L5S1 facet is cleared of all soft tissue and the sacrum is stripped back to the rst dorsal foramen. Complete exposure of all landmarks is critical for accurate screw placement. For positioning of screws in L3, L4, and L5, a line is drawn across the transverse processes and through the
Copyright 2003 Elsevier Science (USA). All rights reserved.
968
SECTION II Spine
Print Graphic
Presentation
FIGURE 3122. A, A 44-year-old woman fell through the attic oor, landed on her buttocks, and sustained this burst fracture. It was an isolated injury; however, the patient had loss of movement and sensation in the lower extremities for approximately 10 minutes after the fall. By the time that she was seen at the trauma center, she had recovered all neurologic function. Computed tomography (B) showed greater than 50% canal compromise, and she had approximately 30 of kyphosis. After discussion of the alternatives, she underwent reduction and xation with two screws above and one below. Intraoperative images (C) showed complete reduction of the deformity. Six months postoperatively, she had lost slight correction of height (D) but achieved solid painless arthrodesis.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
969
inferolateral edge of the facet, as suggested by Roy-Camille and associates128 (Fig. 3125B). Similarly, care must be taken to determine the proper angle of entry into the body. The orientation of the screws at each level is affected by several factors, including the positioning of the patient on the operating table, the amount of kyphotic deformity of the fracture, and the shape of the vertebra. In addition, distortion of the anatomy at the fractured apical level can make accurate placement difcult. Because laminectomy or laminotomy is frequently necessary, direct palpation of the pedicle might be possible and can be helpful in placement. Beginning at the most proximal level, the facet joint is meticulously avoided and entry made through the posterior cortex with a 3-mm oval bur at the inferolateral corner of the pedicle. Such entry requires that the superior screw be angled approximately 15 superiorly toward the end-plate and 10 medially to have it enter through the pedicle. Although most surgeons probe the pedicle when placing pedicle screws during elective fusions, that technique may require signicant force in a young individual with hard bone and an unstable spine. The pedicle can also be drilled with a 2- or 3.2-mm bit until the surgeon has ascertained that the pedicle has been entered. This technique is especially useful when attempting to place a screw in a fractured vertebra. A 2.0-mm drill bit or Kirschner wire is then inserted, with care taken to not place it deeper than the depth of the pedicle. It should not be inserted into the body so that localizing radiographs or uoroscopy can determine the site of entry accurately. Two drill bits at the same level can be reversed if AP and lateral radiographs are being used for
localization, one with the point into the pedicle and one with the point out, so that the position of the two sides can be differentiated (see Fig. 3125C). If image intensication is used, the image should be oriented parallel to the axis of each guide pin. The pin should appear in the inferolateral portion of the pedicle for the superior level and in the center of the pedicle for all other levels. The inferior level is at L5 for an L4 burst fracture and at S1 for an L5 burst fracture. Screw placement at the L5 level is done in a fashion similar to that for the superior end of the construct, with several slight modications. The position of the pedicle is determined in the same manner, although the starting hole for the screw is begun in the center of the pedicle with a high-speed bur to remove the inferior portion of the superior facet of L5. The angle of placement is inward approximately 10 and inferior approximately 15 (parallel to the superior L5 end-plate as the patient is positioned on the table) (see Fig. 3125D). If the inferior screw is to be placed into the sacrum, two options are available. For placement of a screw into the sacral ala, visualization of several landmarks is necessary. The capsule is removed from the L5S1 facet, and the inferior edge of the rst dorsal foramen is exposed. At a point midway between the facet and the rst dorsal foramen, a slight indentation or dimple can be found and is the starting point for insertion of the screw. A 2.0-mm drill bit is placed into the indentation and aligned against the inferior edge of the L5 spinous process (if it exists). Such positioning should orient the drill with 35 of lateral tilt and 25 of inferior tilt (see Fig. 3125E). The posterior cortex of the sacrum is then drilled in that orientation. The
Print Graphic
Presentation
FIGURE 3123. A 63-year-old man sustained a burst fracture of L3. A, A lateral preoperative radiograph demonstrates severe destruction and axial compression of the L3 body. The fracture demonstrates slight posterior translation but little angulation. B, An anteroposterior radiograph demonstrates severe comminution of the vertebral body with spreading of the pedicles and posterior element fractures. C, Computed tomography of the affected level demonstrates the critical radiologic features. Complete comminution of the entire vertebral body is apparent, as well as signicant retropulsion of bone into the canal with nearly complete occlusion of the canal and comminution of the pedicles. Pressure applied to these pedicles would only drive the pedicles into the severely comminuted body and would not cause resultant lordosis and ligamentotaxis.
Copyright 2003 Elsevier Science (USA). All rights reserved.
970
SECTION II Spine
Print Graphic
A
Presentation
FIGURE 3124. Multiple approaches to pedicle screw xation of lumbar fractures may be used. The rst variation is the number of points of xation of the spine. A, Most spinal xators rely on one point of xation above and one point of xation below the level of the fracture and achieve reduction by angulation of the vertebral bodies through the screw xation points. B, Most plate systems, as well as rod-screw systems, have xation at the level above the fracture, at the level below the fracture, and at the fracture level. The second variation is in the direction of sacral xation. C, The xation may be directed into the anterior portion of the S1 body, which is free of both vascular and neural structures. D, Alternatively, the xation may be directed laterally out into the sacral alae and, if taken far enough, likewise lies in a zone free of both neural and vascular elements.
bit is advanced to the anterior cortex of the sacrum simply by pushing it through the soft cancellous bone until the anterior, dense cortical bone of the sacrum is encountered. The anterior cortex is not drilled at this point, but drill bits are placed as described previously, with one inverted, and their position is checked radiographically. On a true lateral view, the drill bit should be oriented parallel to or should slightly converge toward the superior end-plate of the sacrum, approximately 1 cm inferior to it. After checking the position, the hole is overdrilled to a size appropriate for the screw. When drilling the anterior cortex, a hand drill should be used and the drill steadied with both hands to prevent plunging. Once the anterior cortex is felt to be engaged by
the drill bit, three quarters of an additional twist is necessary to penetrate the anterior cortex fully. A depth gauge is used to measure screw length, and care should be taken to medially orient the foot of the depth gauge so that the shortest possible length is used to engage the cortex (the ala slopes laterally, and therefore lateral measurements are always longer). If medial screw orientation into the vertebral body of S1 is necessary for the xation device, the S1 pedicle must be located. An entrance hole is made at the base of the superior facet of S1, and the pedicle is probed and located in standard fashion. Because of the severe medial slope of the sacrum, 20 to 30 of medial and 25 of inferior orientation of the screw are necessary to attain adequate xation in the sacral body.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
971
If the pedicle screw system being used can accommodate xation or requires xation in the apical or fractured level, certain other factors must be considered. First, the conguration of the fractured body must be clearly delineated on the CT scan before attempting screw placement. The most common pattern for L4 and L5 burst fractures is that the superior portion of the body and the pedicle are comminuted but the inferior portion of the pedicle remains attached to the inferior portion of the vertebral body. This pattern can be accompanied by a sagittal split in the body so that the two halves of the vertebra are not attached. Most frequently, however, the area of best screw purchase is in the inferior portion of the body. Therefore, placement requires orientation of the drill bit in a much more inferiorly directed position than normal. In addition, if the two halves are split, a more directly anterior position (rather than medial orientation) might also be necessary for good purchase30 (see Fig. 3125F). A common variation is that one pedicle and the lateral cortex of the body on that side are displaced signicantly. It might not be possible to reduce this injury or place the
nal screw in that pedicle until vertebral height has been restored. Finally, when placing the screws, other cracks and ssures in the body might be palpable as the vertebral body is probed. The surgeon should always be aware of the exact dimensions of that vertebral body and the depth of insertion of any instrument so that the anterior cortex of the body is not penetrated through a fracture line. Screw placement at the fracture level is accomplished in a manner similar to that at other vertebral levels, by opening the posterior cortex over the center of the pedicle with a 3-mm bur. This technique usually requires removal of the inferior portion of the superior facet and probing with a 30 curette before placement of a 2.0-mm drill bit. With all three levels prepared for screw insertion, devices requiring three points of pedicle xation can be applied. Consideration of preparation of the spine for fusion is also necessary before nal insertion of the hardware. Assembly of the construct varies with the system. However, certain principles should be observed independent of the type of system and the number of screws inserted. First, it is critical that the kyphosis be corrected
Print Graphic
Presentation
FIGURE 3125. The operative technique for pedicular xation of low lumbar burst fractures has many similarities from one system to the next. The technique shown emphasizes the critical features. When exposing the spine, care must be taken to not disrupt the interspinous ligament or the facet capsules proximal to the level of instrumentation. In exposing the transverse process opposite the superior pedicle, it is critical that the facet capsule not be disrupted. In view of the location of the pedicle and its proximity to the capsule (A), great care should be taken in this dissection. Screw position can be determined by a number of different techniques. The technique of Roy-Camille (B) positions the entry point at the intersection of a line through the transverse processes and a line through the inferolateral edge of the facet joint. Entry into the pedicle can be facilitated by using a 3-mm oval bur to remove the cortical bone at the location of the suggested entry point. A small probe, sound, or curette can be used to easily traverse the cancellous bone of the pedicle. This technique prevents inadvertent perforation of the pedicle walls. Illustration continued on following page
Copyright 2003 Elsevier Science (USA). All rights reserved.
972
SECTION II Spine
Print Graphic
E
Presentation
F
FIGURE 3125 Continued. Drill bits can be placed into pedicles so that the use of intraoperative image intensication or radiographs will allow identication of the position of the drill bits within the pedicles (C). The orientation of the drill bits within the vertebral bodies changes with the level. In view of the angle of the side wall of L5, the screws should be oriented approximately 10 medially and 15 caudally to accommodate the lordosis of L5 (D). Orientation within the sacrum, as previously described, can be either medially into the body or laterally out into the sacral ala. Lateral orientation requires a 35 lateral tilt and a 25 inferior tilt (E). For a pedicle screw system requiring screw xation into the apical fractured level, a number of specic considerations are necessary. The conguration of the fracture body must be clearly understood before attempting screw placement. If the body is split sagittally, the two halves may be oriented in different directions. Therefore (F), one side may require vertical placement of the screw, whereas the other side, because of orientation, may require slight angulation medially. In addition, the screw may traverse a fracture within the body. The surgeon should feel the fracture site as the screws are placed. A transverse connector is recommended to increase the rigidity of the construct.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
973
before applying distraction. When the fractured level is not instrumented, a straight or slightly contoured rod is inserted into the proximal screw or screws on both sides simultaneously. The rods are locked into the screw or screws in the correct orientation, and then by applying force to both rods either with a rod pusher or by using the reduction devices available with the system, the rods are reduced progressively down into the distal screw heads and preliminarily locked into position. If additional correction of kyphosis is necessary, the rods can be contoured with in situ bending irons. Once correction of the kyphosis has been achieved, the rod is loosened at one end and distraction applied until the interspinous ligament is appropriately tensioned, and then the quality of reduction is checked with image intensication. Additional distraction can be gradually applied while watching for restoration of body height of the fractured level. If a screw is placed in the fractured vertebral level, the method of reduction can be slightly altered. For the Modular system, the central screw has a connector attached to it. Thus, after placing a straight rod and tightening it into the proximal and distal screws, the connector is lengthened to restore lordosis. Other systems also have an ability to apply an anteriorly directed force through the middle screw to achieve reduction. In rod systems without the ability to gradually achieve reduction with the system in place, the rod can be precontoured to the appropriate lordosis and then, for smaller degrees of deformity, either rotated into position similar to correction of scoliosis or attached to the middle and distal screws and reduced into the proximal screw. The reduction process is done in this sequence because most deformity exists at the upper end of the fractured level and the disc space above. Correction of height is done by keeping the middle screw tight and rst loosening the distal screw to allow distraction to be applied across the normal disc space so that it is comparable to the one below. That screw is tightened, and then the proximal screw is loosened and distraction applied across the injured level until it is restored to normal. In most systems it is necessary to thoroughly decorticate the transverse processes and lateral sides of the facets before assembling the construct. Epinephrine-soaked sponges can be used to diminish bleeding. If laminectomy is required, usually only one side of the hardware is assembled, that on the side opposite the surgeon. Partial reduction of the deformity is preferable before laminectomy both to achieve some fracture stability and to attain some fracture reduction if repair of a traumatic dural laceration or removal of a bony fragment is thought necessary. After completing the decompression or repair of the dural laceration, the second side of the construct is placed. The reduction is checked by either radiographic or image intensication; at least one cross lock should be placed, and the bone graft is harvested and placed in the decorticated lateral gutters. Postoperatively, the patient is placed in a regular bed, and either a total-contact or a thoracolumbosacral orthosis, depending on the level of fracture, is applied on approximately the third postoperative day. If a thoracolumbosacral orthosis is used for an L5 fracture or for xation extending to the sacrum, the leg extension is removed at 3
months and the patient is kept in the orthosis for an additional 3 months. The three-screw technique is applicable to L4 and L5 burst fractures in which the body-pedicle junction is intact and to some L3 fractures. It relies on three-point xation for applying slight distraction and lordosis to maintain sagittal alignment. This technique can also be used in patients with burst fractures and comminution of the pedicles at L3, as well as at L4 and L5. Difculty might be encountered with severe comminution of the body or in obtaining solid screw xation. By using the curette, the pedicle nder, and the 2.0-mm drill bit to feel through the pedicle and the body, however, it is possible to obtain reasonable xation in most fractures. Small laminotomies at the apical level can aid in determining the orientation of the pedicle when fractured and in allowing solid xation. Because the major force is a lordotic force at the apical level, satisfactory xation in the pedicle and in some pieces of the body is all that is necessary to maintain three-point xation, which achieves the reduction and rigid xation. For most fractures at L2 and some at L3, xation can be augmented by an additional level of purchase proximally or even, if necessary, an additional level distally with skipping of the fractured level.
Alternative Techniques
Various other techniques have their own advantages and disadvantages. They have been mainly used for the treatment of thoracic and thoracolumbar injuries, with a smaller percentage used for injuries to the upper lumbar area (these were simply included in the overall series). Their applicability is limited when considered for low lumbar (L4 and L5) injuries alone. ROD-BASED INSTRUMENTATION The rst group involves rod-hook instrumentation, which as mentioned previously, has little applicability in the lumbar spine. Straight Harrington distraction rods provide only adjustable distraction for injuries resulting from exion and compression. They have a number of disadvantages for use in the lumbar spine. First, they fail to provide the necessary three-point xation and lordosis or any rotational control.102, 108, 113, 120, 140, 148 They require long lever arms to achieve any reduction, and such length is contraindicated in the lumbar spine. In addition, junctional kyphosis can occur at the proximal end of the instrumented segment as a result of the forces applied to that hook-lamina junction. Because nothing is available to maintain the span of lumbar lordosis and the distance between the posterior elements and the rod, the fracture generally settles into kyphosis when the patient stands. In the lumbar spine, in addition, such instrumentation is complicated by frequent hook dislodgment. The use of sublaminar wires increases the stability, but with a straight rod, it aggravates the loss of lumbar lordosis and contributes to residual kyphosis.51, 64, 112, 144 The length of the instrumented segment has been believed to be a disadvantage of this technique, although the concept of rod longfuse short2, 33 has been used to compensate for that deciency.
Copyright 2003 Elsevier Science (USA). All rights reserved.
974
SECTION II Spine
Contoured rods provide distraction and three-point loading, but they also require accurate contouring, which might require repeated removal and recontouring to achieve optimal reduction. Engagement of the rod in the distal hook is often difcult because of the innate instability of the contoured rod, which has a tendency to rotate to the least stressed position. After assembly of a contoured rod construct, a signicant rotational force is applied to the hook-lamina interface, thus increasing the chance of failure at that location. In addition, in areas with comminution of the apical posterior elements or in which laminectomy is required, no site is available for three-point contact of the central portion of the contour. Hook-rod techniques have limited applicability in lumbar fractures because of the dangers and difculties of hook purchase at the L5 and S1 levels, the necessary end vertebrae for many lumbar rod constructs. The Jacobs rod71 can also be contoured to use in these situations, and its application results in additional stability because of the clamping hooks and rotational control. With any of the multiple hook-rod systems, using only hooks and standard construct length (two levels below and two or three levels above) has the same disadvantages of distal hook placement and long length in the lumbar spine. With multiple hook purchase sites, rigid xation with maintenance of lumbar contours can be achieved, but difculty has been encountered in shortening the construct. Systems with shorter constructs (one below and two above) have the disadvantage of inadequate reduction and laminar fracture and must be supplemented with an anterior procedure to ensure reliability and short length. Preliminary data suggest that the combination of pedicle screws and hooks with this system might be an effective solution to ensure short length of xation and reliability. All these previously mentioned rod-hook systems generally require a minimum of two levels below the fracture and two levels above the fracture, for a total of ve instrumented levels and four interspaces. With laminar comminution, it can be extended to six or seven instrumented levels, but this option is undesirable in the lumbar spine, where the effort to preserve unaffected motion segments is critical. SPINAL PLATES Beginning with the work of Louis93 and that of RoyCamille and associates,128 systems of spinal plates xed with pedicle screws have been used for fractures. These systems have subsequently been modied by Steffee and colleagues141 and by Luque. Even currently, Louis plates92 are being advocated for use in the stabilization of spinal trauma. The strength of these plates lies in the fact that they can achieve rigid xation of the spine with limited length of instrumentation. Roy-Camille plates for the lumbar spine allow two pedicle screws to be placed at each level in the large pedicles of the low lumbar spine. Similarly, they allow instrumentation at the apical level. Their shortcoming is that they rely on postural reduction for achieving reduction. They essentially plate the fracture in situ rather than applying pedicle screws in optimal position and then achieving reduction. In injuries with
severe malalignment or rotational instability, difculty might be encountered in placing adjacent levels so that the screws line up with the plate at all levels. The plates are best restricted to low lumbar fractures, although they have been used by many for the treatment of upper lumbar and thoracolumbar spine fractures. The risk of missing the pedicle during insertion of the screw, however, increases as the pedicle diameter becomes smaller and as the thoracolumbar junction is approached; hence the value in comparison with that of rod xation decreases. Plate systems such as the Steffee (VSP)4, 5, 39, 96, 149 have been used for both thoracolumbar and lumbar fractures. However, signicant loss of correction has been identied in patients with marked body comminution. Better results are achieved in low lumbar fractures without signicant deformity or by augmenting the anterior column with a strut graft. Plate systems allow direct decompression, stabilization, and fusion in the absence of severe deformity. ANTERIOR DECOMPRESSION AND FIXATION Anterior surgical techniques are most benecial for late direct decompression and stabilization of low lumbar fractures. Fractures in the lumbar spine from L2 to L5 can be visualized through a retroperitoneal approach, which is relatively straightforward. The technique allows excellent exposure to the vertebral bodies and the certainty of complete anterior decompression. In the acute trauma setting, the role of anterior surgery in the lumbar spine is somewhat less clear. The risks and complexity of direct anterior decompression and stabilization need to be balanced against the relative risks of the posterior surgery. In the lumbar spine, it has been demonstrated that the use of an anterior strut graft alone to reconstruct the spine is inadequate and results in anterior compression of the graft and kyphotic deformities. This complication can be avoided by applying posterior stabilization at the same sitting or by the use of some adjunctive anterior procedure. Use of the Kaneda device73 or anterior plating6, 52, 69 for neutralization can augment the results and achieve more rigid xation, and these measures are adequate for long-term stabilization. Care must be taken that the devices do not protrude against the aorta, or vascular complications can arise.15 The technique of retroperitoneal dissection and direct anterior decompression has been described in Chapter 30; it is essentially the same for the low lumbar spine. Dissection of L4 and especially L5 requires extreme care in handling the iliac vein. FLEXION-DISTRACTION INJURIES The two most common types of exion-distraction injuries are Chance fractures (and related variants) and bilateral facet dislocation. As previously noted, the relative incidence of these two types of injury is reversed in the lumbar spine in comparison with the thoracolumbar junction. Flexion-distraction fractures, as classied by Gumley and associates58 and by Gertzbein and Court-Brown,55 are not generally amenable to any distraction techniques for stabilization. Fractures that traverse the spinous process, pedicle, and body can often be reduced in a hyperexten-
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
975
FIGURE 3126. A, Lateral radiograph of a exion-distraction injury in a 17-year-old boy. The use of an internal spinal xator with screw xation at the levels above and below the injury allows both correction of kyphosis and restoration of vertebral height. B, The xation device relies on the strength of the spinal screw to resist cantilever bending and therefore requires full reduction of the spinal deformity into slight lordosis to place the weight-bearing axis of the spine over the instrumentation. Residual kyphosis would place the weight-bearing axis anteriorly and thus accentuate cantilever bending and encourage early screw failure.
Print Graphic
Presentation
sion cast and heal predictably. Those that cannot be reduced, however, and that will result in signicant residual lumbar kyphosis should undergo surgical reduction and stabilization. In addition, fractures that traverse the posterior ligamentous complex, pedicle, and body commonly result in ligamentous instability after fracture healing and should undergo stabilization and fusion initially for an optimal result. Both these injury types can be treated with a posterior compression construct because of the absence of posterior wall comminution and disc involvement. Depending on the involvement of the posterior elements, the compression instrumentation requires two levels (one interspace) or three levels (two interspaces) (Fig. 3126). The technique used can involve a rod-hook system, such as Harrington compression or Cotrel-Dubousset, TSRH, or most commonly a pedicle screw system. When the fracture line traverses the interspinous ligament and the posterior elements are left intact, the injury can be stabilized with a single-level construct. When pedicle xation is considered, purchase in the fractured pedicle and body must be carefully assessed if two-level xation is chosen (Fig. 3127). The most common exion-distraction injury in the thoracolumbar spine is bilateral facet dislocation. This injury is distinctly rare in the lumbar spine but requires special consideration. Such injuries can result in severe posterior ligament and disc disruption. Patients with lumbar spine and lumbosacral dislocations tend to have incomplete neural injuries and thus increased potential for recovery. A tendency to consider the use of a one-level compression construct to save levels in the lumbar spine should be discouraged. An L2L3 bilateral facet dislocation should therefore be directly reduced, and a one-level neutralization construct with pedicle xation used to limit
the length of xation. Because the disc disruption is so signicant with this injury, if a single-level compression construct is used, extruded disc material might actually cause signicant neural compression and additional decit, either centrally or at either root. Bilateral facet dislocations in the upper lumbar spine can also be treated satisfactorily with a one- or two-level pedicle screw construct. This technique is extremely straightforward because the posterior elements and posterior wall of both vertebral bodies are intact. Once the facets have been reduced, screws are placed in the pedicles of the level above and below the dislocation (assuming that no body fractures are present) and connected by a straight rod. Lordosis is achieved rst and then just enough distraction applied to place the vertebral levels in normal orientation and the disc at normal height. Compression should not be used. Care should be taken during reduction of the bilateral facet dislocation so that the facets are not damaged, because they contribute signicantly to the stability of the construct. Operative reduction of dislocated facets can be achieved with the following method: After complete delineation of the dislocated facets by meticulous dissection, the disrupted facet capsules and ligamentum avum are resected. A laminar spreader is placed between the two spinous processes and gentle distraction applied until the tips of the facets are unlocked (Fig. 3128A). The laminar spreader is twisted slightly to reduce the facet and then released to allow the facets to be reduced into normal position. An interspinous wire (18 gauge) is placed around the two spinous processes to complete the reduction (see Fig. 3128B). The spine is now reduced and stabilized, and a short rod-sleeve technique or pedicle screw construct can be applied to complete the construct. At the end of the procedure, the interspinous wire can be left in
Copyright 2003 Elsevier Science (USA). All rights reserved.
976
SECTION II Spine
place or removed. A multiple hook/rod construct can also be used if length is not a primary concern (upper lumbar spine). Other techniques that can maintain the reduction with a short xation length and without the use of compression can also be effective. In the low lumbar spine, where conservation of levels is important and a one-level construct is considered, prophylactic discectomy should be performed before a single-level compression construct. This procedure removes damaged disc material, prevents extrusion, and allows the use of a single-level compression construct. Specically, an L4L5 facet dislocation can be stabilized with a single-level L4L5 compression construct and the proximal and distal levels left open. SHEAR INJURIES AND COMPLEX DEFORMITIES The optimal stabilization construct for shear injuries and complex deformities generally involves posterior stabilization, which with an operative plan allows stabilization of the various deforming forces. Each one needs to be individualized for the particular situation. Segmental
xation is often necessary to control the abnormal forces, especially in patients with stiff spines (see Figs. 3117 and 3118). Other constructs20 have been used with success; however, the more points of xation, the greater the degree of stability that can be achieved with these injuries.
Complications of Surgical Treatment
NEUROLOGIC DETERIORATION Neurologic deterioration can occur intraoperatively and postoperatively. It has been demonstrated that a patients lumbar spine is not well immobilized on a Stryker frame. As the patient rolls from a prone to a supine position, an unstable burst fracture can shift signicantly, which could result in increased neurologic damage. Long-term immobilization on a logrolling frame can also cause shifting of fragments and potential neural damage. This situation is one indication for early surgical intervention. Intraoperative neurologic deterioration can be caused by applying distraction over a kyphotic segment of the lumbar spine, thus stretching the already tight neural elements over a prominent area. Reduction of kyphosis should be accomplished before any distraction maneuver. In addition, passing sublaminar wires or any xation device in the canal at the apical level of the kyphosis and deformity can involve the risk of increased neurologic decit secondary to placing objects in an already tight canal. Hook placement at L5 and S1 can also result in neurologic decit because the very small canal and the severely lordotic lumbosacral junction can place the shoe of the hook in a position to compress the dural sac. Postoperative neurologic complications can be caused by dislodgment of anterior grafts or by recurrence of deformity. Placement of pedicle screws may be associated with either root decit or more severe decits, depending on the degree of error in placement (Fig. 3129). NONUNION Nonunion of lumbar spine fractures is a frequent complication that has been reported in as many as 40% of fractures at the lumbosacral junction. More rigid xation techniques with segmental xation, as well as meticulous fusion techniques, are required to prevent this complication. Care must be taken to extend bone graft proximally above the upper hook in a rod construct to the transverse process on that side to achieve solid arthrodesis. In addition, with bulky posterior hardware, care must be taken that the device does not obscure pertinent areas for bony fusion. LOSS OF CORRECTION
Print Graphic
Presentation
FIGURE 3127. A 17-year-old girl sustained a Chance fracture of L4 and had exion instability after nonoperative treatment. A posterior compression construct was able to reduce the kyphosis and eliminate the instability. One-level compression instrumentation can be used acutely in exion-distraction injuries with posterior instability, but the purchase in the fractured body must be carefully assessed if a two-level/oneinterspace construct is chosen.
Most reports on spinal injury have noted loss of correction, as well as residual kyphosis. This complication is related to the inability of the xation system selected to achieve rigid xation that does not change with the patients position. Proper selection of hardware and meticulous application with concern for counteracting deforming forces can minimize loss of correction.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures
977
Print Graphic
Presentation
A
FIGURE 3128. Reduction of a bilateral facet dislocation in the lumbar spine should be able to be accomplished in a controlled fashion with preservation of the facets to allow reestablishment of stability. Dissection of the soft tissues is accomplished, and the facet dislocations are identied. The ruptured ligamentum avum is removed, as are the disrupted facet capsules. Cartilage is removed from the superior facet of the lower level under direct vision. A laminar spreader is then placed between the two spinous processes and gently manipulated until the facets are distracted. When the tips of the facets are disengaged, the laminar spreader is tipped to push the inferior facet anteriorly and pull the superior facets posteriorly. The distraction on the laminar spreader is then released to allow the facets to engage in a normal position. A, An interspinous wire is placed across the involved level and tightened to complete the reduction and reestablish stability. A short rod-sleeve construct can then be applied. B, The slight distraction applied by the rod-sleeve construct does not cause redislocation because the primary force is lordosis, which counteracts the exion moment of the original injury.
Copyright 2003 Elsevier Science (USA). All rights reserved.
978
SECTION II Spine 9. Argenson, C.; Lovet, J.; de Peretti, F et al. Treatment of spinal .; fractures with Cotrel-Dubousset instrumentation. Results of the rst 85 cases. Poster exhibit presented at the Scoliosis Research Society, Amsterdam, September 1989. 10. Asher, M.; Strippgen, W. Anthropometric studies of the human sacrum relating to dorsal transsacral implant design and development. Clin Orthop 203:5862, 1986. 11. Bedbrook, G.M. Treatment of thoracolumbar dislocation and fractures with paraplegia. Clin Orthop 112:2743, 1975. 12. Benson, D.R.; Burkus, J.K.; Montesano, P.X.; et al. Unstable thoracolumbar and lumbar burst fractures treated with an AO Fixateur Interne. J Spinal Disord 5:335343, 1992. 13. Benzel, E.C.; Ball, P.A. Management of low lumbar fractures by dorsal decompression, fusion, and lumbosacral laminar distraction xation. J Neurosurg 92(Suppl):142148, 2000. 14. Boucher, M.; Bhandari, M.; Kwok, D.; Health related quality of life after short segment instrumentation of lumbar burst fractures. J Spinal Disord 14:417426, 2001. 15. Brown, L.P.; Bridwell, K.H.; Holt, R.T.; et al. Aortic erosions and lacerations associated with the Dunn anterior spinal instrumentation. Orthop Trans 10:16, 1986. 16. Bucholz, R.W.; Gill, K. Classication of injuries to the thoracolumbar spine. Orthop Clin North Am 17:6773, 1986. 17. Cain, J.E.; DeJong, J.T.; Dinenberg, A.S.; et al. Pathomechanical analysis of thoracolumbar burst fracture reduction. Spine 18:1647 1654, 1993. 18. Carl, A.L.; Tromanhauser, S.C.; Roger, D.J. Pedicle screw instrumentation for thoracolumbar burst fractures and fracturedislocations. Spine 17(Suppl):317324, 1992. 19. Chakera, T.M.H.; Bedbrook, G.; Bradley, C.M. Spontaneous resolution of spinal canal deformity after burst-dispersion fracture. AJNR Am J Neuroradiol 9:779785, 1988. 20. Chaloupka, R. Complete rational burst fracture of the third lumbar vertebra managed by posterior surgery. Spine 24:302305, 1999. 21. Chan, D.P.K.; Seng, N.K.; Kaan, K.T. Nonoperative treatment in burst fractures of the lumbar spine (L2-L5) without neurologic decits. Spine 18:320325, 1993. 22. Chance, G.Q. Note on a type of exion fracture of the spine. Br J Radiol 21:452453, 1948. 23. Chapman, J.R.; Anderson, P.A. Thoracolumbar spine fractures with neurologic decit. Orthop Clin North Am 25:595612, 1994. 24. Clohisy, J.C.; Akbarnia, B.A.; Bucholz, R.D.; et al. Neurologic recovery associated with anterior decompression of spine fractures at the thoracolumbar junction (T12-L1). Spine 17(Suppl):325330, 1992. 25. Comissa, F Eismont, F Green, B.H. Dural laceration occurring .P.; .J.; with burst fractures and associated laminar fractures. J Bone Joint Surg Am 71:10441052, 1989. 26. Court-Brown, C.M.; Gertzbein, S.D. The management of burst fractures of the fth lumbar vertebra. Spine 12:308312, 1987. 27. Crutcher, J.P.; Anderson, P.A.; King, H.A.; et al. Indirect spinal canal decompression in patients with thoracolumbar burst fractures treated by posterior distraction rods. J Spinal Disord 4:3948, 1991. 28. Dai, L.Y. Remodeling of the spinal canal after thoracolumbar burst fractures. Clin Orthop 382:119123, 2001. 29. Davis, A.A.; Carragee, E.J. Bilateral facet dislocation at the lumbosacral joint. Spine 18:25402544, 1993. 30. De Boeck, H.; Opdecam, P. Split coronal fractures of the lumbar spine. Treatment by posterior internal xation and transpedicular bone grafting. Int Orthop 23(2):8790, 1999. 31. Dehner, J.R. Seatbelt injuries of the spine and abdomen. AJR Am J Roentgenol 111:833843, 1971. 32. De Klerk, L.W.L.; Fontijne, W.P.J.; Stijnen, T.; et al. Spontaneous remodeling of the spinal canal after conservative management of the thoracolumbar burst fractures. Spine 23:10571060, 1998. 33. Dekutoski, M.B.; Conlan, S.; Salciccioli, G.G. Spinal mobility and deformity after Harrington rod stabilization and limited arthrodesis of thoracolumbar fractures. J Bone Joint Surg Am 75:168176, 1993. 34. Denis, F The three-column spine and its signicance in the . classication of acute thoracolumbar spinal injuries. Spine 8:817 831, 1983. 35. Denis, F Spinal instability as dened by the three-column spine . concept in acute spinal trauma. Clin Orthop 189:6576, 1984.
Print Graphic
Presentation
FIGURE 3129. Although segmental xation with pedicle screws can shorten the construct and more rigidly x the lumbar lordosis, the surgical technique is more exacting. Especially in a traumatized spine, where normal landmarks may be obscured, misplacement of screws (arrow) is a potential complication.
SUMMARY
zzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzz Treatment of lumbar fractures requires an understanding of the mechanics and normal functioning of the lumbar spine. Hardware selection depends on the goals to be achieved, the time to surgery, and the types of instabilities encountered. Appropriate consideration of the treatment goals for an individual patient and the injury leads to optimal results. The surgeons selection of treatment should not be based on knowledge of a single technique, but rather on knowledge of the relative advantages and disadvantages of various nonoperative and operative procedures for the treatment of lumbar spine fractures.
REFERENCES 1. Akbarnia, B.A.; Moskowicz, A.; Merenda, J.T.; et al. Surgical treatment of thoracic spine fractures with Cotrel-Dubousset instrumentation. Poster exhibit presented at the Scoliosis Research Society, Amsterdam, September 1989. 2. Akbarnia, B.A.; Crandall, D.G.; Burkus, K.; et al. Use of long rods and a short arthrodesis for burst fractures of the thoracolumbar spine. J Bone Joint Surg Am 76:16291635, 1994. 3. Albert, T.J.; Levine, M.J.; An, H.S. Concomitant noncontiguous thoracolumbar and sacral fractures. Spine 18:12851291, 1994. 4. An, H.S.; Vaccaro, A.; Cotler, J.M.; et al. Low lumbar burst fractures. Comparison among body cast, Harrington rod, Luque rod, and Steffee plate. Spine 16(Suppl):440444, 1991. 5. An, H.S.; Simpson, J.M.; Ebraheim, N.A.; et al. Low lumbar burst fractures: Comparison between conservative and surgical treatments. Orthopedics 15:367373, 1992. 6. An, H.S.; Tae-Hong, L.; Jae-Won, Y.; et al; Biomechanical evaluation of anterior thoracolumbar spinal instrumentation. Spine 20:1979 1983, 1995. 7. Anderson, P.A.; Rivara, F Maier, R.V.; et al. The epidemiology of .P.; seatbelt-associated injuries. J Trauma 31:6067, 1991. 8. Andreychik, D.; Alander, D.; Senica, K.; Stauffer, S. Burst fractures of the 2nd through the 5th lumbar vertebrae. J Bone Joint Surg Am 78:11561166, 1996.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures 36. Denis, F Burkus, J.K. Diagnosis and treatment of cauda equina .; entrapment in the vertebral lamina fracture of lumbar burst fractures. Spine 16(Suppl):433439, 1991. 37. Dick, W. The Fixateur Interne as a versatile implant for spine surgery. Spine 12:882900, 1987. 38. Doerr, T.E.; Montesano, P.X.; Burkus, J.K.; et al. Spinal canal decompression in traumatic thoracolumbar burst fractures: Posterior distraction rods versus transpedicular screw xation. J Orthop Trauma 5:403411, 1991. 39. Ebelke, D.K.; Asher, M.A.; Neff, J.R.; et al. Survivorship analysis of VSP spine instrumentation in the treatment of thoracolumbar and lumbar burst fractures. Spine 16(Suppl):428432, 1991. 40. Edwards, C.C.; Levine, A.M. Early rod sleeve stabilization of the injured thoracic and lumbar spine. Orthop Clin North Am 17:121145, 1986. 41. Elliot, H.C. Cross-sectional diameters and areas of the human spinal cord. Anat Rec 93:287293, 1945. 42. Epstein, N.E.; Epstein, J.A. Limbus lumbar vertebral fractures in 27 adolescents and adults. Spine 16:962966, 1991. 43. Esses, S.I.; Botsford, D.J.; Wright, T.; et al. Operative treatment of spinal fractures with the AO internal xator. Spine 16(Suppl):146 150, 1991. 44. Ferguson, R.L.; Allen, B.L., Jr. A mechanistic classication of thoracolumbar spine fractures. Clin Orthop 189:7788, 1984. 45. Fidler, M.W.; Plasmas, C.M.T. The effects of ve types of support on the segmental mobility of the lumbosacral spine. J Bone Joint Surg Am 65:943947, 1983. 46. Finn, C.A.; Stauffer, E.S. Burst fracture of the fth lumbar vertebra. J Bone Joint Surg Am 74:398403, 1992. 47. Fletcher, B.D.; Brogdon, B.G. Seatbelt fractures of the spine and sternum. JAMA 200:167168, 1967. 48. Frankel, H.L. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. Paraplegia 7:179192, 1969. 49. Frederickson, B.E.; Yuan, H.A.; Miller, H. Burst fractures of the fth lumbar vertebra. J Bone Joint Surg Am 64:10881094, 1982. 50. Frederickson, B.E.; Edwards, W.T.; Rauschning, W.; et al. Vertebral burst fractures: An experimental, morphologic, and radiographic study. Spine 17:10121021, 1992. 51. Gaines, R.W.; Breedlove, R.; Munson, G. Stabilization of thoracic and thoracolumbar fracture dislocations with Harrington rods and sublaminar wires. Clin Orthop 189:195203, 1984. 52. Gardner, V.O.; Thalgott, J.S.; White, J.I. The contoured anterior spinal plate system (CASP). Indications, techniques, and results. Spine 19:550555, 1994. 53. Garrett, J.W.; Braunstein, P.W. Seatbelt syndrome. J Trauma 2:220237, 1962. 54. Gellad, F .E.; Levine, A.M.; Joslyn, J.N.; et al. Pure thoracolumbar facet dislocation: Clinical features and CT appearance. Radiology 161:505508, 1986. 55. Gertzbein, S.D.; Court-Brown, C.M. Flexion-distraction injuries of the lumbar spine: Mechanisms of injury and classication. Clin Orthop 227:5260, 1988. 56. Graziano, G.P. Cotrel-Dubousset hook and screw combination for spine fractures. J Spinal Disord 6:380385, 1993. 57. Greenbaum, E.; Harris, L.; Halloran, W.X. Flexion fracture of the lumbar spine due to lap-type seatbelts. Cal Med 113:7476, 1970. 58. Gumley, G.; Taylor, T.K.; Ryan, M.D. Distraction fractures of the lumbar spine. J Bone Joint Surg Br 64:520525, 1982. 59. Gurwitz, G.S.; Dawson, J.M.; McNamera, M.J.; et al. Biomechanical analysis of three surgical approaches for lumbar burst fractures using short-segment instrumentation. Spine 18:977982, 1993. 60. Haddad, G.H.; Zickel, R.E. Intestinal perforation and fracture of the lumbar spine caused by lap-type seatbelt. N Y J Med 67:930932, 1967. 61. Handel, S.F Twiford, T.W., Jr.; Reigel, D.H.; et al. Posterior lumbar .; apophyseal fractures. Radiology 13:629633, 1979. 62. Hardaker, W.T.; Cook, W.A.; Freidman, A.H.; et al. Bilateral transpedicular decompression and Harrington rod stabilization in the management of severe thoracolumbar burst fractures. Spine 17:162171, 1992. 63. Harrington, R.M.; Budorick, T.; Hoyt, J.; et al. Biomechanics of indirect reduction of bone retropulsed into the spinal canal in vertebral fracture. Spine 18:692699, 1993.
979
64. Herring, J.A.; Wenger, D.R. Segmental spinal instrumentation: A preliminary report of 40 consecutive cases. Spine 7:285298, 1983. 65. Holdsworth, F Fractures, dislocations and fracture-dislocations .W. of the spine. J Bone Joint Surg Am 52:15341551, 1970. 66. Holdsworth, F .W.; Hardy, A. Early treatment of paraplegia from fractures of the thoracolumbar spine. J Bone Joint Surg Br 35:540550, 1953. 67. Howland, W.J.; Curry, J.L.; Bufngton, C.B. Fulcrum fractures of the lumbar spine. JAMA 193:240241, 1965. 68. Hu, S.S.; Capen, D.A.; Rimolda, R.L.; et al. The effect of surgical decompression on neurologic outcome after lumbar fractures. Clin Orthop 288:166173, 1993. 69. Huang, T.J.; Chen, J.Y.; Shih, H.N. et al. Surgical indications in low lumbar burst fractures: Experience with anterior locking plate system and the reduction-xation system. J Trauma 39:910914, 1995. 70. Huelke, D.F Kaufer, H. Vertebral column injuries and seatbelts. .; J Trauma 15:304318, 1975. 71. Jacobs, R.R.; Casey, M.P. Surgical management of thoracolumbar spinal injuries: General principles and controversial considerations. Clin Orthop 189:2235, 1984. 72. Jeanneret, B.; Ho, P.K.; Magerl, F Burst-shear exion-distraction . injuries of the lumbar spine. J Spinal Disord 6:473481, 1993. 73. Kaneda, K.; Abumi, K.; Fijiya, M. Burst fractures with neurologic decits of the thoracolumbar-lumbar spine: Results of anterior decompression with anterior instrumentation. Spine 9:788795, 1984. 74. Knight, R.Q.; Stornelli, D.P.; Chan, D.P.K.; et al. Comparison of operative versus nonoperative treatment of lumbar burst fractures. Clin Orthop 293:112121, 1993. 75. Kostiuk, J.P.; Munting, E.; Valdevit, A. Biomechanical analysis of screw load sharing in pedicle xation of the lumbar spine. J Spinal Disord 7:394401, 1994. 76. Krag, M.H.; Beynnon, B.D.; Pope, M.H.; et al. An internal xator for posterior application to short segments of the thoracic, lumbar or lumbosacral spine: Design and testing. Clin Orthop 203:7588, 1986. 77. Krag, M.H.; Weaver, D.L.; Beynnon, B.D.; Haugh, B.D. Morphometry of the thoracic and lumbar spine related to transpedicular screw placement for surgical spinal xation. Spine 13:2732, 1988. 78. Kreitz, B.G.; Cote, P.; Cassidy, J.D. L5 vertebral compression fracture: A series of ve cases. J Manipulative Physiol Ther 18(2):9197, 1995. 79. Krompinger, W.J.; Frederickson, B.E.; Mino, D.E.; Yuan, H.A. Conservative management of fractures of the thoracic and lumbar spine. Clin Orthop 17:161170, 1986. 80. Lagrone, M.O.; Bradford, D.S.; Moe, J.H.; et al. Treatment of symptomatic atback after spinal fusion. J Bone Joint Surg Am 70:569580, 1988. 81. Lemons, V.R.; Wagner, F .C.; Montesane, P.X. Management of thoracolumbar fractures with accompanying neurological injury. Neurosurgery 30:667671, 1992. 82. Levine, A.M.; Edwards, C.C. Lumbar spine trauma. In: Camins, M.; OLeary, P., eds. The Lumbar Spine. New York, Raven, 1987, pp. 185212. 83. Levine, A.M.; Edwards, C.C.; Gellad, F Indirect decompression . of the spinal canal in the thoracolumbar spine. American Spinal Injury Association, Abstracts Digest, March 2022, 1987, pp. 1618. 84. Levine, A.M.; Edwards, C.C. Low lumbar burst fractures. Reduction and stabilization using the modular spine xation system. Orthopedics 11:14271432, 1988. 85. Levine, A.M.; Bosse, M.; Edwards, C.C. Bilateral facet dislocations in the thoracolumbar spine. Spine 13:630640, 1988. 86. Levine, A.M. The surgical treatment of low lumbar fractures. Semin Spine Surg 2:4153, 1990. 87. Levine, A.M. Dural lacerations in low lumbar burst fractures. Paper presented at the American Academy of Orthopaedic Surgeons meeting, Washington, D.C., February 1992. 88. Levine, A.M. The long term follow-up of patients with L4 and L5 burst fractures treated with surgical stabilization. Submitted for publication. 89. Lewis, J.; McKibbin, B. The treatment of unstable fracturedislocations of the thoracolumbar spine accompanied by paraplegia. J Bone Joint Surg Br 56:603612, 1974.
Copyright 2003 Elsevier Science (USA). All rights reserved.
980
SECTION II Spine 115. Nevitt, M.C.; Ross, P.D.; Palermo, L.; et al. Association of prevalent vertebral fractures, bone density, and alendronate treatment with incident vertebral fractures: Effect of number and spinal location of fractures. Bone 25:613619, 1999. 116. Norton, P.L.; Brown, T. The immobilizing efciency of back braces. J Bone Joint Surg Am 39:111131, 1957. 117. OCallaghan, J.P.; Ullrich, C.G.; Yuan, H.A.; et al. CT of facet distraction in exion injuries of the thoracolumbar spine: The naked facet. AJNR Am J Neuroradiol 1:97102, 1980. 118. Olerud, S.; Karlstrom, G.; Sjostrom, L. Transpedicular xation of thoracolumbar vertebral fractures. Clin Orthop 227:4451, 1988. 119. Olinger A.; Hildebrant, U.; Mutshler, W.; Menger, M.D. First clinical experience with an endoscopic retroperitoneal approach for anterior fusion of lumbar spine fractures from levels T12 to L5. Surg Endosc 13:12151219, 1999. 120. Panjabi, M.M.; Abumi, K.; Duranceau, J.S. Three-dimensional stability of thoracolumbar fractures stabilized with eight different instrumentations. Trans Orthop Res Soc 12:458, 1987. 121. Panjabi, M.M.; Oda, T.; Wang, J.-L. The effects of pedicle screw adjustments on neural spaces in burst fracture surgery. Spine 25:16371643, 2000. 122. Parker, J.W.; Lane, J.R.; Karaikovic, E.E.; Gains, R.W. Injuries of the thoracolumbar spine associated with restraint use in head-on motor vehicle accidents. J Spinal Disord 13:297304, 2000. 123. Rauschning, W. Correlative multiplanar computed tomographic anatomy of the normal spine. In: Post, J.D., ed. Computed Tomography of the Spine. Baltimore, Williams & Wilkins, 1984, pp. 2067. 124. Rechtine, G.R. 2nd.; Cahill, D.; Chrin, A.M. Treatment of thoracolumbar trauma: Comparison of complications of operative versus nonoperative treatment. J Spinal Disord 12:406409, 1999. 125. Rennie, W.; Mitchell, N. Flexion distraction fractures of the thoracolumbar spine. J Bone Joint Surg Am 55:386390, 1973. 126. Ritchie, W.P., Jr.; Ersek, R.A.; Bunch, W.L.; et al. Combined visceral and vertebral injuries from lap-type seatbelts. Surg Gynecol Obstet 131:431435, 1970. 127. Rogers, I.F The roentgenographic appearance of transverse or . Chance fractures of the spine: The seatbelt fracture. AJR Am J Roentgenol 111:844849, 1971. 128. Roy-Camille, R.; Saillant, G.; Mazel, C. Plating of thoracic, thoracolumbar and lumbar injuries with pedicle plates. Orthop Clin North Am 17:147159, 1986. 129. Saillant, G. Etude anatomique des pedicles, vertebreau, application chirurgicales. Rev Chir Orthop Traumatol 62:151160, 1976. 130. Sasso, R.C.; Cotler, H.B.; Reuben, J.D. Posterior xation of thoracic and lumbar spine fractures using DC plates and pedicle screws. Spine 16(Suppl):134139, 1991. 131. Scoles, P.V.; Linton, A.E.; Latimer, B.; et al. Vertebral body and posterior element morphology: The normal spine in middle life. Spine 13:10821086, 1988. 132. Seybold, E.A.; Sweeny, C.A.; Fredrickson, B.E.; et al. Functional outcome of low lumbar burst fractures: A multicenter review of operative and nonoperative treatment of L3-L5. Spine 24:2154 2161, 1999. 133. Shen, W.J.; Liu, T.J.; Shen, Y.S. Nonoperative treatment versus posterior xation for thoracolumbar junction burst fractures without neurologic decit. Spine 26:10381045, 2001. 134. Shiba, K.; Katsuki, M.; Ueta, T.; et al. Transpedicular xation with Zielke instrumentation in the treatment of thoracolumbar and lumbar injuries. Spine 19:19401949, 1994. 135. Shuman, W.P.; Rogers, J.V.; Sickler, M.E.; et al. Thoracolumbar burst fractures: CT dimensions of the spinal canal relative to postsurgical improvement. AJR Am J Roentgenol 145:337341, 1985. 136. Sjostrom, L.; Jacobsson, O.; Karlstrom, G.; et al. Spinal canal remodeling after stabilization of thoracolumbar burst fractures. Eur Spine J 3:312317, 1994. 137. Slosar, P.J.; Patwardhan, A.G.; Lorenz, M.; et al. Instability of the lumbar burst fracture and limitations of transpedicular instrumentation. Spine 20:14521461, 1995. 138. Smith, W.S.; Kaufer, H. Patterns and mechanisms of lumbar injuries associated with seatbelts. J Bone Joint Surg Am 51:239 254, 1969. 139. Stagnara, P.; De Mauroy, J.C.; Dran, G.; et al. Reciprocal angulation of vertebral bodies in a sagittal plane: Approach to references for the evaluation of kyphosis and lordosis. Spine 7:335342, 1982.
90. Lindahl, S.; Willen, J.; Nordwall, A.; et al. The crush-cleavage fracture: A new thoracolumbar unstable fracture. Spine 8:559 569, 1983. 91. Lindsey, R.W.; Dick, W. The Fixateur Interne in the reduction and stabilization of thoracolumbar spine fractures in patients with neurologic decit. Spine 16(Suppl):140145, 1991. 92. Louis, C.A.; Gauthier, V.Y.; Louis, R.P. Posterior approach with Louis plates for fractures of the thoracolumbar and lumbar spine with and without neurologic decits. Spine 23:20302040, 1998. 93. Louis, R. Fusion of the lumbar and sacral spine by internal xation with screw plates. Clin Orthop 203:1833, 1986. 94. Magerl, F External skeletal xation of the lower thoracic and .P. lumbar spine. In: Uhthoff, H.K., ed. Current Concepts of External Fixation of Fractures. New York, Springer-Verlag, 1982, pp. 353366. 95. Magerl, F Stabilization of the lower thoracic and lumbar spine .P. with external skeletal xation. Clin Orthop 189:125141, 1984. 96. Maiman, D.J.; Pintar, F Yoganandan, N.; et al. Effects of anterior .; vertebral grafting on the traumatized lumbar spine after pedicle screw-plate xation. Spine 18:24232430, 1993. 97. Mann, K.A.; Found, E.M.; Yuan, H.A.; et al. Biomechanical evaluation of the effectiveness of anterior spinal xation systems. Orthop Trans 11:378, 1987. 98. Markel, D.C.; Graziano, G.P. A comparison study of treatment of thoracolumbar fractures using the Ace posterior segmental xator and Cotrel-Dubousset instrumentation. Orthopedics 18:679686, 1995. 99. Marsh, H.O.; Bailey, D. Chance fractures caused by seatbelts: Presentation of three cases. J Kans Med Soc 71:361365, 1970. 100. Marshall, D.; Johnell, O.; Wedel, H. Meta-analysis of how well measures of bone mineral density predict occurrences of osteoporotic fractures. BMJ 312:12541259, 1996. 101. McAfee, P.C.; Yuan, H.A.; Frederickson, B.E.; et al. The value of computed tomography in thoracolumbar fractures. An analysis of one hundred consecutive cases and a new classication. J Bone Joint Surg Am 65:461473, 1983. 102. McAfee, P.C.; Werner, F .W.; Glisson, R.R. A biomechanical analysis of spinal instrumentation systems in thoracolumbar fractures. Spine 10:204217, 1985. 103. McAfee, P.C.; Bohlman, H.H.; Yuan, H.A. Anterior decompression of traumatic thoracolumbar fractures with incomplete neurologic decit using a retroperitoneal approach. J Bone Joint Surg Am 67:89104, 1985. 104. McLain, R.F Sparling, E.; Benson, D.R. Early failure of short.; segment pedicle instrumentation for thoracolumbar fractures. J Bone Joint Surg Am 75:162167, 1993. 105. Melton, L.J. III; Lane, A.W.; Cooper, C.; et al. Prevalence and incidence of vertebral deformities. Osteoporos Int 3:113119, 1993. 106. Micheli, L.J. Low back pain in the adolescent: Differential diagnosis. Am J Sports Med 7:362364, 1979. 107. Mick, C.A.; Carl, A.; Sachs, B.; et al. Burst fractures of the fth lumbar vertebra. Spine 18:18781884, 1993. 108. Mino, D.E.; Stauffer, E.S.; Davis, P.K.; et al. Torsional loading of Harrington distraction rod instrumentation compared to segmental sublaminar and spinous process supplementation. Orthop Trans 9:119, 1985. 109. Mirkovic, S.; Abitbol, J.J.; Steinman, J.; et al. Anatomic consideration for sacral screw placement. Spine 16(Suppl):289294, 1991. 110. Miyakoshi, N.; Abe, E.; Shimada, Y; et al. Anterior decompression with single segmental spinal interbody fusion for lumbar burst fractures. Spine 24:6773, 1999. 111. Mumford, J.; Weinstein, J.N.; Spratt, K.F et al. Thoracolumbar .; burst fractures. Spine 18:955970, 1993. 112. Munson, G.; Satterlee, C.; Hammond, S.; et al. Experimental evaluation of Harrington rod xation supplemented with sublaminar wires in stabilizing thoracolumbar fracture dislocations. Clin Orthop 189:97102, 1984. 113. Nagel, D.A.; Koogle, T.A.; Piziale, R.C.; et al. Stability of the upper lumbar spine following progressive disruptions and the application of individual internal and external xation devices. J Bone Joint Surg Am 63:6270, 1981. 114. Neumann, A.; Nordwall, A.; Osvalder, A.L. Traumatic instability of the lumbar spine. Spine 20:11111121, 1995.
Copyright 2003 Elsevier Science (USA). All rights reserved.
CHAPTER 31 Low Lumbar Fractures 140. Stauffer, E.S.; Neil, J.L. Biomechanical analysis of structural stability of internal xation in fractures of the thoracolumbar spine. Clin Orthop 112:159164, 1975. 141. Steffee, A.D.; Biscup, R.S.; Sitkowski, D.J. Segmental spine plates with pedicle screw xation. Clin Orthop 203:4553, 1986. 142. Stephens, G.C.; Devito, D.P.; McNamara, M.J. Segmental xation of lumbar burst fractures with Cotrel-Dubousset instrumentation. J Spinal Disord 5:344348, 1992. 143. Stromsoe, K.; Hem, E.S.; Auanan, E. Unstable vertebral fractures in the lower third of the spine treated with closed reduction and transpedicular posterior xation: A retrospective analysis of 82 fractures in 78 patients. Eur Spine J 6:239244, 1997. 144. Sullivan, J.A. Sublaminar wiring of Harrington distraction rods for unstable thoracolumbar spine fractures. Clin Orthop 189:178185, 1984. 145. Takata, K.; Shum-Ichi, I.; Kazuhisa, T. Fracture of the posterior margin of a lumbar vertebral body. J Bone Joint Surg Am 70:589594, 1988. 146. Viale, G.L.; Silvestro, C.; Francaviglia, N.; et al. Transpedicular decompression and stabilization of burst fractures of the lumbar spine. Surg Neurol 40:104, 1993. 147. Vornanen, M.J.; Bostman, O.M.; Myllynen, P.J. Reduction of bone retropulsed into the spinal canal in thoracolumbar vertebral body compression burst fractures. Spine 20:16991703, 1995. 148. Ward, J.J.; Nasca, R.J.; Lemons, J.E.; et al. Cyclic tortional testing of Harrington and Luque spinal implants. Orthop Trans 9:118, 1985. 149. Weyns, F Rommens, P.M.; Van Calenbergh, F et al. Neurological .; .; outcome after surgery for thoracolumbar fractures. A retrospective
981
150. 151. 152. 153.
154.
155. 156. 157. 158.
study of 93 consecutive cases, treated with dorsal instrumentation. Eur Spine J 3:276281, 1994. White, A.A.; Panjabi, M.M. The basic kinematics of the spine: A review of past and current knowledge. Spine 3:1220, 1978. White, A.A.; Panjabi, M.M. Clinical Biomechanics of the Spine. Philadelphia, J.B. Lippincott, 1978. Whitesides, T.E. Traumatic kyphosis of the thoracolumbar spine. Clin Orthop 128:7992, 1977. Wildburger, R.; Mahring, M.; Paszicsnyek, T.; et al. Dorsal stabilization of thoracolumbar spinal instability. Comparison of three different implantation systems. Arch Orthop Trauma Surg 113:244247, 1994. Willen, J.; Lindahl, S.; Irstam, I.; et al. Unstable thoracolumbar fractures: A study by CT and conventional roentgenology of the reduction effect of Harrington instrumentation. Spine 9:214219, 1984. Winter, R.B. Congenital Deformities of the Spine. New York, Thieme-Stratton, 1983. Yuan, H.A.; Garn, S.R.; Dickman, C.A.; et al. A Historical cohort study of pedicle screw xation in thoracic, lumbar, and sacral spinal fusions. Spine 19(Suppl):22792296, 1994. Zindrick, M.R.; Wiltsie, L.L.; Doornik, A.; et al. Analysis of the morphometric characteristics of the thoracic and lumbar pedicles. Spine 12:160166, 1987. Zou, D.; Yoo, J.U.; Edwards, T.; et al. Mechanics of anatomic reduction of thoracolumbar burst fractures. Spine 18:195203, 1993.
Copyright 2003 Elsevier Science (USA). All rights reserved.
Copyright 2003 Elsevier Science (USA). All rights reserved.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- (Morrissy & Stein Atlas of Pediatric Orthopaedics Surgery (3rd Edition)Document2 pages(Morrissy & Stein Atlas of Pediatric Orthopaedics Surgery (3rd Edition)nhieuntn0% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- (Rang) Children's Fractures (2nd Edition)Document2 pages(Rang) Children's Fractures (2nd Edition)nhieuntn0% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- (Morrissy & Stein Lovell & Winter's Pediatric Orthopaedics (5th Edition)Document2 pages(Morrissy & Stein Lovell & Winter's Pediatric Orthopaedics (5th Edition)nhieuntn0% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- (Beaty & Kasser) Rockwood & Wilkins' Fractures in Children (5th Edition)Document2 pages(Beaty & Kasser) Rockwood & Wilkins' Fractures in Children (5th Edition)nhieuntnNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- CH 41Document41 pagesCH 41nhieuntnNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- (Blount) Fractures in ChildrenDocument288 pages(Blount) Fractures in ChildrennhieuntnNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- CH 40Document48 pagesCH 40nhieuntnNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- CH 33Document8 pagesCH 33nhieuntnNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- CH 25Document25 pagesCH 25nhieuntnNo ratings yet
- CH 39Document48 pagesCH 39nhieuntnNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- CH 36Document57 pagesCH 36nhieuntnNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- CH 35Document22 pagesCH 35nhieuntnNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- CH 37Document42 pagesCH 37nhieuntnNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- CH 38Document116 pagesCH 38nhieuntn100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- CH 34Document17 pagesCH 34nhieuntnNo ratings yet
- CH 30Document69 pagesCH 30nhieuntnNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- CH 32Document21 pagesCH 32nhieuntnNo ratings yet
- CH 27Document31 pagesCH 27nhieuntnNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- CH 29Document61 pagesCH 29nhieuntnNo ratings yet
- CH 23Document9 pagesCH 23nhieuntnNo ratings yet
- CH 26Document38 pagesCH 26nhieuntnNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CH 28Document37 pagesCH 28nhieuntnNo ratings yet
- CH 24Document13 pagesCH 24nhieuntnNo ratings yet
- CH 19Document24 pagesCH 19nhieuntnNo ratings yet
- CH 17Document10 pagesCH 17nhieuntnNo ratings yet
- CH 22Document22 pagesCH 22nhieuntnNo ratings yet
- CH 21Document34 pagesCH 21nhieuntnNo ratings yet
- CH 20Document98 pagesCH 20nhieuntnNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- CH 18Document46 pagesCH 18nhieuntnNo ratings yet
- Prof. DR. Aboe Amar Joesoef, DR, Sp.S. (K)Document44 pagesProf. DR. Aboe Amar Joesoef, DR, Sp.S. (K)Ryan FeizalNo ratings yet
- Orthopedic Clinics Na 2007 Vol 38 ScoliosisDocument102 pagesOrthopedic Clinics Na 2007 Vol 38 ScoliosisChanina BlacksteinNo ratings yet
- Nursing Diagnosis Rationale Interventions Rationale EvaluationDocument2 pagesNursing Diagnosis Rationale Interventions Rationale EvaluationJobie CasipongNo ratings yet
- Advanced Mechanical VentilationDocument96 pagesAdvanced Mechanical VentilationMukhtar KhanNo ratings yet
- Huntingtons DiseaseDocument9 pagesHuntingtons Diseaseapi-320253549No ratings yet
- Junard M. Lu Hap, RN: #51 Champaca Lapu-Lapu Street Brgy. Dadiangas East, General Santos City Contact Number 050-310-9586Document6 pagesJunard M. Lu Hap, RN: #51 Champaca Lapu-Lapu Street Brgy. Dadiangas East, General Santos City Contact Number 050-310-9586Junard M. Lu HapNo ratings yet
- Review Notes 2000 - CardiologyDocument58 pagesReview Notes 2000 - Cardiologyeliaszavaleta100% (1)
- Nefrolitiasis RadiologiDocument9 pagesNefrolitiasis RadiologiSteven SetioNo ratings yet
- Down Syndrome Article 1Document3 pagesDown Syndrome Article 1api-252032417No ratings yet
- Student Nurses' Community: Nursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesStudent Nurses' Community: Nursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale EvaluationVen Belista86% (14)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nclex 2Document147 pagesNclex 2Habet Fidem100% (5)
- Physician Assisted Suicide (Pros & Cons, Arguments For and Against, Advantages & Disadvantages of Euthanasia or Doctor-Assisted Suicice)Document5 pagesPhysician Assisted Suicide (Pros & Cons, Arguments For and Against, Advantages & Disadvantages of Euthanasia or Doctor-Assisted Suicice)Lyana MahaliNo ratings yet
- 12 Little Known Facts About CoffeeDocument3 pages12 Little Known Facts About CoffeeBulgare de SoareNo ratings yet
- Pressure Ulcers - Prevention and Management of Pressure Ulcers StrategyDocument38 pagesPressure Ulcers - Prevention and Management of Pressure Ulcers StrategyAlex Alexandra AlexNo ratings yet
- Discussion RsovDocument30 pagesDiscussion RsovwarholeblackNo ratings yet
- Multiple Choice QuestionsDocument8 pagesMultiple Choice QuestionsSouravSenguptaNo ratings yet
- PQCNC New Initiative Proposal CLABSIDocument17 pagesPQCNC New Initiative Proposal CLABSIkcochranNo ratings yet
- FCL ReflectionDocument6 pagesFCL ReflectionCJ AngelesNo ratings yet
- Person of Interest S02E07 720p Bluray demaNDDocument48 pagesPerson of Interest S02E07 720p Bluray demaNDJack CooperNo ratings yet
- Endodontic Diagnostic Terminology UpdateDocument3 pagesEndodontic Diagnostic Terminology UpdateAlyaefkageNo ratings yet
- Lethal Triad in Trauma: Michael K Howlett MD Associate Professor Dept of Emergency Medicine Dalhousie UniversityDocument31 pagesLethal Triad in Trauma: Michael K Howlett MD Associate Professor Dept of Emergency Medicine Dalhousie Universitymuhammad ajiNo ratings yet
- Fluid and ElectrolytesDocument14 pagesFluid and Electrolytesstring44100% (2)
- Hospital &/or Medical Centre - ChecklistDocument2 pagesHospital &/or Medical Centre - ChecklistRiddhimaNo ratings yet
- Clonidine HydrochlorideDocument1 pageClonidine HydrochlorideLovelyn Joy Abubo CortezNo ratings yet
- Interview FormDocument3 pagesInterview FormCamelia IonasNo ratings yet
- TransferEndorsementForm PDFDocument1 pageTransferEndorsementForm PDFBryan BarredoNo ratings yet
- Fundamentals of Nursing Test II QuestionsDocument14 pagesFundamentals of Nursing Test II QuestionsclobregasNo ratings yet
- Hospital Pharmacy Training AssignmentDocument24 pagesHospital Pharmacy Training AssignmentSathish SatzzNo ratings yet
- Cerebral Palsy - Critical Elements of CareDocument25 pagesCerebral Palsy - Critical Elements of CaremarkoNo ratings yet
- Psychiatric NursingDocument39 pagesPsychiatric Nursingjeshema100% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (29)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)