You might also like
- Lo Que Tratamos y Lo Que EstudiamosDocument13 pagesLo Que Tratamos y Lo Que EstudiamosCarlos Alan LopezNo ratings yet
- Key Recommendations GuidelinesDocument56 pagesKey Recommendations GuidelinesCarlos Alan Lopez100% (1)
- Iecas y Ara2Document8 pagesIecas y Ara2Carlos Alan LopezNo ratings yet
- Ebook - Just The Facts2008Document6 pagesEbook - Just The Facts2008Carlos Alan LopezNo ratings yet
- Diferencias de Guias American As y EuropeasDocument10 pagesDiferencias de Guias American As y EuropeasCarlos Alan LopezNo ratings yet
- Ebook - Fisiopato Braunwald Cardio - 2Document2 pagesEbook - Fisiopato Braunwald Cardio - 2Carlos Alan Lopez100% (1)
- Ebook - Cecil Ed23 - 2Document3 pagesEbook - Cecil Ed23 - 2Carlos Alan Lopez100% (3)
- IECASDocument14 pagesIECASCarlos Alan Lopez100% (1)
- Diagnostico HF 2004Document8 pagesDiagnostico HF 2004Carlos Alan Lopez100% (1)
- Nuevas y Tradicionales AproximacionesDocument14 pagesNuevas y Tradicionales AproximacionesCarlos Alan LopezNo ratings yet
- MyPyramid AnatomyDocument1 pageMyPyramid AnatomyCarlos Alan LopezNo ratings yet
- Ob GdlnsDocument262 pagesOb Gdlnsapi-3728652No ratings yet
- Ebook - Fisiopato Braunwald CardioDocument2 pagesEbook - Fisiopato Braunwald CardioCarlos Alan LopezNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- A Presentation On Fibre Identification Test and YarnDocument22 pagesA Presentation On Fibre Identification Test and YarnSMJV AATLNo ratings yet
- Table - Diseases Notifiable To The OIEDocument1 pageTable - Diseases Notifiable To The OIEЂорђе100% (1)
- Colonial Downs Harnesss Tip Sheet Thursday Sep13Document1 pageColonial Downs Harnesss Tip Sheet Thursday Sep13EZ HorsePlayNo ratings yet
- Teacher: Jose Acuña: Ana Paula Viera RamosDocument1 pageTeacher: Jose Acuña: Ana Paula Viera RamosVIERA RAMOS ANA PAULANo ratings yet
- Pyhylum Chordata: "An Overview of Chordates"Document10 pagesPyhylum Chordata: "An Overview of Chordates"shriyans4269No ratings yet
- Blaszkowski Et Al v. Mars Inc. Et Al - Document No. 390Document7 pagesBlaszkowski Et Al v. Mars Inc. Et Al - Document No. 390Justia.comNo ratings yet
- Karel CapekDocument67 pagesKarel CapekJasmina Pavlic100% (3)
- Room On The BroomDocument31 pagesRoom On The BroomHebing WuNo ratings yet
- Poultry Pocketbook 2017Document27 pagesPoultry Pocketbook 2017Dulce AmorNo ratings yet
- This That These Those Grammar Drills 44826Document2 pagesThis That These Those Grammar Drills 44826Nicolás RuizNo ratings yet
- Evolution and Biodiversity Test ReviewDocument15 pagesEvolution and Biodiversity Test ReviewSanaa SamkoNo ratings yet
- HOOTER by Nicky Epstein PDFDocument3 pagesHOOTER by Nicky Epstein PDFAnneita100% (1)
- Wa0106.Document6 pagesWa0106.Priscila FreitasNo ratings yet
- Parasitology TableDocument9 pagesParasitology TablehumanupgradeNo ratings yet
- Discover MARDIDocument33 pagesDiscover MARDIMARDI Scribd75% (4)
- Control de Lectura TortulentaDocument3 pagesControl de Lectura TortulentaMonicaFaunesNo ratings yet
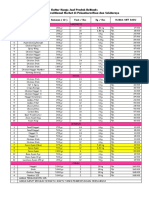
- Daftar Harga Jual Produk Belfoods Untuk Grosir, Traditional Market Di Pekanbaru-Riau Dan SekitarnyaDocument2 pagesDaftar Harga Jual Produk Belfoods Untuk Grosir, Traditional Market Di Pekanbaru-Riau Dan SekitarnyaDwi Mahendra SubhiNo ratings yet
- Organ Systems and Their FunctionsDocument15 pagesOrgan Systems and Their FunctionsNoemi Lyn CastilloNo ratings yet
- 2018 BortoDocument26 pages2018 BortoBortoNo ratings yet
- Physical Death of Jesus Christ Jam A 1986Document10 pagesPhysical Death of Jesus Christ Jam A 1986Silvester SikoraNo ratings yet
- Homeopathy Provings of Boa ConstrictorDocument18 pagesHomeopathy Provings of Boa Constrictoraruen79No ratings yet
- Aeneid 4.129-183Document5 pagesAeneid 4.129-183melanieshoeNo ratings yet
- Reticular FormationDocument26 pagesReticular Formationsr_sushilNo ratings yet
- Mastitis NotesDocument42 pagesMastitis NotesCristina CarvalhoNo ratings yet
- 24a44 Environment Part 1 Compressed - 1320066 103 115 PDFDocument13 pages24a44 Environment Part 1 Compressed - 1320066 103 115 PDFAbhay kumar SinghNo ratings yet
- A Busy Mom's Guide To Daily Meal Preparation: I Just Wanted To Expound That What I Usually Do IsDocument8 pagesA Busy Mom's Guide To Daily Meal Preparation: I Just Wanted To Expound That What I Usually Do IsCarina TanNo ratings yet
- Rampokan MacanDocument8 pagesRampokan MacanAnneke JulianitaNo ratings yet
- Module DLP ANSWERSDocument9 pagesModule DLP ANSWERSStephanie PhangNo ratings yet
- 01 MorphologyDocument52 pages01 MorphologyGhina Verina LermanNo ratings yet
- 74 Cue Card AnsDocument167 pages74 Cue Card Ansduaa fatimaNo ratings yet