You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Anti-Microbial Therapy Final With AlarmsDocument245 pagesAnti-Microbial Therapy Final With AlarmsMahmoud Ahmed MahmoudNo ratings yet
- Fetal Malnutrition: DR. Mahmoud Ahmed Mahmoud Ahmed Faculty of Medicine Alexandria UniversityDocument11 pagesFetal Malnutrition: DR. Mahmoud Ahmed Mahmoud Ahmed Faculty of Medicine Alexandria UniversityMahmoud Ahmed MahmoudNo ratings yet
- Investigative HepatologyDocument24 pagesInvestigative HepatologyMahmoud Ahmed MahmoudNo ratings yet
- Fetal MalnutritionDocument2 pagesFetal MalnutritionMahmoud Ahmed MahmoudNo ratings yet
- Ovarian Hyperstimulation SyndromeDocument3 pagesOvarian Hyperstimulation SyndromeMahmoud Ahmed MahmoudNo ratings yet
- Non-Ischemic Central Retinal Vein OcclusionDocument17 pagesNon-Ischemic Central Retinal Vein OcclusionMahmoud Ahmed MahmoudNo ratings yet
- Investigative HepatologyDocument6 pagesInvestigative HepatologyMahmoud Ahmed MahmoudNo ratings yet
- Non-Ischemic Central Retinal Vein OcclusionDocument6 pagesNon-Ischemic Central Retinal Vein OcclusionMahmoud Ahmed MahmoudNo ratings yet
- Livor MortisDocument16 pagesLivor MortisMahmoud Ahmed MahmoudNo ratings yet
- Livor MortisDocument5 pagesLivor MortisMahmoud Ahmed MahmoudNo ratings yet
- Branch Retinal Vein Occlusion (BRVO)Document4 pagesBranch Retinal Vein Occlusion (BRVO)Mahmoud Ahmed MahmoudNo ratings yet
- Management of AgitationDocument8 pagesManagement of AgitationMahmoud Ahmed MahmoudNo ratings yet
- Drug Management of AgitationDocument14 pagesDrug Management of AgitationMahmoud Ahmed MahmoudNo ratings yet
- Diphtheria VaccineDocument5 pagesDiphtheria VaccineMahmoud Ahmed MahmoudNo ratings yet
- Phylum Platyhelminths (Flat Worms)Document2 pagesPhylum Platyhelminths (Flat Worms)Mahmoud Ahmed MahmoudNo ratings yet
- Iphtheria Accine Oxoid: Mahmoud Ahmed Mahmoud 846Document23 pagesIphtheria Accine Oxoid: Mahmoud Ahmed Mahmoud 846Mahmoud Ahmed MahmoudNo ratings yet
- Endoscopic Surgery For Cancer LarynxDocument11 pagesEndoscopic Surgery For Cancer LarynxMahmoud Ahmed MahmoudNo ratings yet
- A-Autonomic Drugs: 1) CholinergicDocument28 pagesA-Autonomic Drugs: 1) CholinergicMahmoud Ahmed MahmoudNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- TR-SENSES MercadoDocument174 pagesTR-SENSES MercadoroseNo ratings yet
- WFNS Neuroanatomy Committee 3rd WebinarDocument4 pagesWFNS Neuroanatomy Committee 3rd WebinarhalikalifhayaNo ratings yet
- Four Corners Second Edition - Level 2 - U2VocabularyDocument3 pagesFour Corners Second Edition - Level 2 - U2VocabularyVoice Of AnkaraNo ratings yet
- Medical Surgical Nursing PinoyDocument67 pagesMedical Surgical Nursing Pinoyalfred31191% (23)
- Anatomy of The Ear: Prof. Dr. Mohamed Talaat EL - GhonemyDocument46 pagesAnatomy of The Ear: Prof. Dr. Mohamed Talaat EL - Ghonemyadel madanyNo ratings yet
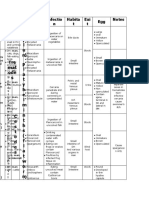
- Cranial Nerves TableDocument1 pageCranial Nerves TablePIOZRNo ratings yet
- Year 2 NeuroDocument111 pagesYear 2 NeuroShahi GhaniNo ratings yet
- Demir 2019Document7 pagesDemir 2019ashaNo ratings yet
- 聲音研究Document54 pages聲音研究roselee0214No ratings yet
- RPD ReviewDocument24 pagesRPD ReviewAnoush ZamaniNo ratings yet
- Theme: The Human Brain. Brain Technology: Grade 11Document13 pagesTheme: The Human Brain. Brain Technology: Grade 11Umitzhan RustembekovaNo ratings yet
- CNS DevelopmentDocument158 pagesCNS DevelopmentMubashir SiyalNo ratings yet
- Anatomy MCQ - Head & Neck PDFDocument20 pagesAnatomy MCQ - Head & Neck PDFسماح صلاح100% (3)
- Normal Radiographic Anatomical Landmarks: Master Day2Document75 pagesNormal Radiographic Anatomical Landmarks: Master Day2Rabab BuKhamseenNo ratings yet
- Carnaby Videofluoroscopic Data SheetDocument4 pagesCarnaby Videofluoroscopic Data SheetKanky Espinoza RuizNo ratings yet
- Algoritmo para El Tto Defectos NasalesDocument14 pagesAlgoritmo para El Tto Defectos NasalesNicolás Silva GalvisNo ratings yet
- Functional and Neuroanatomical Bases of Developmental Stuttering: Current InsightsDocument17 pagesFunctional and Neuroanatomical Bases of Developmental Stuttering: Current InsightsDai ArhexNo ratings yet
- Ent Operative NotesDocument8 pagesEnt Operative NoteshawairyNo ratings yet
- 426 C1 MCQ'sDocument5 pages426 C1 MCQ'sKholoud Kholoud100% (1)
- Past MCQs On Ocular AnatomyDocument7 pagesPast MCQs On Ocular AnatomyEliza Spark40% (5)
- Anatomy and Physiology of Respiratory SystemDocument9 pagesAnatomy and Physiology of Respiratory SystemLiza Marie Cayetano AdarneNo ratings yet
- Fetal SkullDocument40 pagesFetal Skullsapana shah100% (1)
- Laryngomalacia - PPTX Dr. FeriDocument114 pagesLaryngomalacia - PPTX Dr. FeriAldy BimaNo ratings yet
- Giai Phau Mach Mau NaoDocument40 pagesGiai Phau Mach Mau NaoHoàng Bùi TháiNo ratings yet
- TOMAC An Orthognathic Treatment Planning System Part 1 Soft Tissue AnalysisDocument9 pagesTOMAC An Orthognathic Treatment Planning System Part 1 Soft Tissue Analysis허성수No ratings yet
- Productos La 1Document6 pagesProductos La 1Anderson GarzonNo ratings yet
- Brodmann Areas 1Document1 pageBrodmann Areas 1rienz nicnic peraltaNo ratings yet
- Orthognathic DR Shruthi PDFDocument54 pagesOrthognathic DR Shruthi PDFShruthee KNo ratings yet
- Salivary Gland McqsDocument6 pagesSalivary Gland McqsQuranSunnat100% (1)
- Intraoral Periapical AnatomyDocument77 pagesIntraoral Periapical AnatomyNeama HussienNo ratings yet