You might also like
- Last Minute Embryology: Human embryology made easy and digestible for medical and nursing studentsFrom EverandLast Minute Embryology: Human embryology made easy and digestible for medical and nursing studentsNo ratings yet
- The Amnion and Amniotic FluidDocument7 pagesThe Amnion and Amniotic FluidMerina FirmansahNo ratings yet
- Stem CellsDocument15 pagesStem CellsDelia Andreia ȘveduneacNo ratings yet
- Sin Título 2Document16 pagesSin Título 2Anilu ApNo ratings yet
- Physiology of Amniotic Fluid Volume RegulationDocument8 pagesPhysiology of Amniotic Fluid Volume RegulationYosep SutandarNo ratings yet
- Amniotic PhysioDocument3 pagesAmniotic PhysiobjfieroNo ratings yet
- Hydra Mi NosDocument8 pagesHydra Mi NosSudha DeviNo ratings yet
- Amniotic Fluid As A Vital Sign For Fetal Wellbeing: ReviewDocument9 pagesAmniotic Fluid As A Vital Sign For Fetal Wellbeing: ReviewMeska AmeliaNo ratings yet
- Fetal Membranes IMBBSDocument26 pagesFetal Membranes IMBBSSubham YadavNo ratings yet
- Romzan Alfiriza R (2018) Maryo Juan L.T (2018) Sarah Safrilia (201810401011007)Document22 pagesRomzan Alfiriza R (2018) Maryo Juan L.T (2018) Sarah Safrilia (201810401011007)SarahNo ratings yet
- 2006 7 E292-E299 William M. Gilbert: Amniotic Fluid DynamicsDocument10 pages2006 7 E292-E299 William M. Gilbert: Amniotic Fluid DynamicsMel MurNo ratings yet
- Pathologies of The Amniotic Fluid: Gyneco Naji HajjDocument13 pagesPathologies of The Amniotic Fluid: Gyneco Naji HajjHassan KawtharanyNo ratings yet
- Fetal MembranesDocument17 pagesFetal MembranesQaiser InayatNo ratings yet
- Anatomy and Embryology of Umbilicus in Newborns ADocument8 pagesAnatomy and Embryology of Umbilicus in Newborns AAubrey PerezNo ratings yet
- Amniotic Fluid Water Dynamics: M.H. Beall, J.P.H.M. Van Den Wijngaard, M.J.C. Van Gemert, M.G. RossDocument8 pagesAmniotic Fluid Water Dynamics: M.H. Beall, J.P.H.M. Van Den Wijngaard, M.J.C. Van Gemert, M.G. RossCorín AnelNo ratings yet
- Amniotic FluidDocument33 pagesAmniotic FluidElsa Aprillia SujadiNo ratings yet
- Wvith: ExchangedDocument10 pagesWvith: ExchangedJessica StephanieNo ratings yet
- OLIGOHIDRAMNIOSDocument20 pagesOLIGOHIDRAMNIOSJorge Luis Sánchez AlarcónNo ratings yet
- Perkembangan Plasenta (Autosaved) .En - IdDocument18 pagesPerkembangan Plasenta (Autosaved) .En - IdFATIMAHNo ratings yet
- 11th Lecture Amnion& Amniotic FluidDocument35 pages11th Lecture Amnion& Amniotic FluidHussein Al Saedi100% (1)
- Balance de Agua en El Feto y El Recién NacidoDocument5 pagesBalance de Agua en El Feto y El Recién NacidoCarlos ReveloNo ratings yet
- Selaput EmbrioDocument25 pagesSelaput EmbrioMartupa SidabutarNo ratings yet
- Pathophysiology Hidrop FetalisDocument25 pagesPathophysiology Hidrop FetalisPandu Nugroho KantaNo ratings yet
- Amniocentrices (From The Greek Amnion For "Sac" and KenteDocument5 pagesAmniocentrices (From The Greek Amnion For "Sac" and KenteJohn Paolo Tamayo OrioNo ratings yet
- Amniotic FluidDocument55 pagesAmniotic FluidRoselle Joy D. RosalejosNo ratings yet
- Stages of Fetal Growth and DevelopmentDocument10 pagesStages of Fetal Growth and DevelopmentGrant KhangabNo ratings yet
- Embryology, Yolk Sac - StatPearls - NCBI BookshelfDocument10 pagesEmbryology, Yolk Sac - StatPearls - NCBI Bookshelfr9fch8mws7No ratings yet
- Fetal Membranes and PlacentaDocument48 pagesFetal Membranes and Placentaveegeer100% (4)
- Fallopian Tube PresentationDocument41 pagesFallopian Tube PresentationReena Ross Nathan100% (3)
- CA RationaleDocument8 pagesCA RationaleNursing LectureNo ratings yet
- Amnion 1Document2 pagesAmnion 1Oryza SativaniNo ratings yet
- Extraembryonic MembraneDocument41 pagesExtraembryonic MembraneDangkoNo ratings yet
- Sofie R Krisnadi, Dr. SpogDocument82 pagesSofie R Krisnadi, Dr. SpogYogi OktiandiNo ratings yet
- Anatomy and Physiology FinalDocument2 pagesAnatomy and Physiology FinalChloé Jane Hilario100% (1)
- Fertilization: Glora P. de Leon, RN, RM, ManDocument103 pagesFertilization: Glora P. de Leon, RN, RM, ManJoan VillafrancaNo ratings yet
- SAQ EmbryologyDocument9 pagesSAQ EmbryologyShilpa DuttaNo ratings yet
- Picture of The Month: What Is Amniotic Fluid Sludge'?Document6 pagesPicture of The Month: What Is Amniotic Fluid Sludge'?Luis InostrozaNo ratings yet
- Disorders in Amniotic FluidDocument5 pagesDisorders in Amniotic FluidLatansa DinaNo ratings yet
- Embryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesDocument13 pagesEmbryology, Pathophysiology, and Ultrasound Characteristics of The Placenta ObjectivesAudrey100% (5)
- Extra-Embryonic MembranesDocument60 pagesExtra-Embryonic MembranesDaniel MendozaNo ratings yet
- TTN AafpDocument9 pagesTTN Aafpsiti nur rachmaniNo ratings yet
- Amniotic FluidDocument7 pagesAmniotic FluidCherralaine CorderoNo ratings yet
- Anatomy and Embryology of Umbilicus in Newborns: A Review and Clinical CorrelationsDocument7 pagesAnatomy and Embryology of Umbilicus in Newborns: A Review and Clinical Correlationsbayu pamungkasNo ratings yet
- OB Definition of TermsDocument9 pagesOB Definition of TermsWarrenSandovalNo ratings yet
- PlacentaDocument11 pagesPlacentasubashikNo ratings yet
- Extraembryonic MembranesDocument4 pagesExtraembryonic MembranesShafiullah Habib LitonNo ratings yet
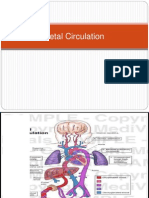
- Fetal CirculationDocument28 pagesFetal CirculationNelai GoNo ratings yet
- Mere A: SyncytiotrophoblastDocument6 pagesMere A: SyncytiotrophoblastMere MujeresNo ratings yet
- FertilizationDocument6 pagesFertilizationKristine Castillo100% (1)
- Congenital Abnormalities of The UterusDocument7 pagesCongenital Abnormalities of The Uterusمحمود الموسويNo ratings yet
- Transient Tachypnea of The Newborn: Pediatrics in Review December 2008Document10 pagesTransient Tachypnea of The Newborn: Pediatrics in Review December 2008Haneen Dabbas2019No ratings yet
- Neo-Natal Physiology and Post-Natal AdaptationsDocument27 pagesNeo-Natal Physiology and Post-Natal Adaptationskiflie derejeNo ratings yet
- Fertilization and Fetal DevelopmentDocument50 pagesFertilization and Fetal DevelopmentMark Ludwig Labastida100% (1)
- EmbryologyDocument26 pagesEmbryologyBryan Mae H. Degorio100% (1)
- Amniotic Fluid and Cord Abnormalities: DR - Saswati Tripathy Professor ObgyDocument46 pagesAmniotic Fluid and Cord Abnormalities: DR - Saswati Tripathy Professor ObgySaranya BalamuruganNo ratings yet
- NCLEX Review of Maternity NursingDocument34 pagesNCLEX Review of Maternity NursingAlain Chery100% (2)
- Bovine Reproduction Booklet UK A5 16pp Text 10Document20 pagesBovine Reproduction Booklet UK A5 16pp Text 10lenn chandNo ratings yet
- Unit 2 - Fertilization, Impantation, Development of Placenta and Its Function, AbnormalityDocument62 pagesUnit 2 - Fertilization, Impantation, Development of Placenta and Its Function, AbnormalityN. Siva100% (1)
- OSCE On 14/3/2008: Describe Gynaecoid PelvisDocument82 pagesOSCE On 14/3/2008: Describe Gynaecoid PelvisKahing LiNo ratings yet
- A. Paracervical Block C. Give Spinal Block D. Pudendal BlockDocument48 pagesA. Paracervical Block C. Give Spinal Block D. Pudendal BlockMae Rose Charlene MendozaNo ratings yet
- Amniotic Fluid DisordersDocument22 pagesAmniotic Fluid Disordersvictor onapaNo ratings yet
- Hilaria Sas 8Document3 pagesHilaria Sas 8Christy Mae Batucan HilariaNo ratings yet
- Post MaturityDocument5 pagesPost MaturityBa BamNo ratings yet
- GRP 7 Partograph BSN - 2DDocument13 pagesGRP 7 Partograph BSN - 2DCzarina Mae Quinones Tadeo0% (1)
- High Risk Pregnancy Part 2Document12 pagesHigh Risk Pregnancy Part 2Kenneth Noveno100% (1)
- Case Study On Breech BirthDocument65 pagesCase Study On Breech BirthSujan Shrestha94% (32)
- MCN Lec Fetal DevpDocument580 pagesMCN Lec Fetal DevpknotstmNo ratings yet
- Case 5Document41 pagesCase 5Trisha Mae Marquez100% (2)
- Fertilization & Fetal DevelopmentDocument23 pagesFertilization & Fetal DevelopmentDimple CosNo ratings yet
- OB FC Nov 2021 NLEDocument9 pagesOB FC Nov 2021 NLEAlyssa SaibiNo ratings yet
- Lesson Plan Preparing For Parenthood Pregnancy and Labor-1Document12 pagesLesson Plan Preparing For Parenthood Pregnancy and Labor-1Ting AlqNo ratings yet
- A Clinical Study On Oligohydramnios in The ThirdDocument23 pagesA Clinical Study On Oligohydramnios in The ThirdDickyNo ratings yet
- Midterm NotesDocument28 pagesMidterm NotesGen FranchesKyle Cortez ErigbuagasNo ratings yet
- Physical Examination For OBDocument63 pagesPhysical Examination For OBQuolette Constante87% (77)
- Maternal & Child Nursing: NNCM 107 Lilia B. DungalaDocument176 pagesMaternal & Child Nursing: NNCM 107 Lilia B. DungalaagentcasperNo ratings yet
- Case StudyDocument5 pagesCase StudyJui Perano100% (2)
- Amniotiv Fluid DisorderDocument22 pagesAmniotiv Fluid DisorderLiangkiuwiliu100% (1)
- AmniocentesisDocument10 pagesAmniocentesisDane Orilla100% (1)
- AbbreviationsDocument7 pagesAbbreviationsPallaviNo ratings yet
- Chapter 26Document84 pagesChapter 26Johanna Erazo Padilla100% (1)
- 648-672 CH21 Lowdermilk PDFDocument25 pages648-672 CH21 Lowdermilk PDFMark Anthony EspirituNo ratings yet
- Nursing Staff Development DepartmentDocument15 pagesNursing Staff Development DepartmentJohnmer AvelinoNo ratings yet
- TerminologyDocument38 pagesTerminologypandem soniyaNo ratings yet
- Amniotic Fluid DisordersDocument16 pagesAmniotic Fluid DisordersLytiana Williams100% (2)
- Partogram Case StudiesDocument6 pagesPartogram Case StudiesnyangaraNo ratings yet
- Assessment of Fetal Lung MaturityDocument16 pagesAssessment of Fetal Lung MaturitybenNo ratings yet
- Maternal and Child NursingDocument11 pagesMaternal and Child NursingKSY JanedoeNo ratings yet
- Partograph: By. Ronalyn A. Fabrigas, RN., MN Credits ToDocument36 pagesPartograph: By. Ronalyn A. Fabrigas, RN., MN Credits ToJmarie Brillantes Popioco100% (1)
- Research Article Risk Factors For Meconium Stained Amniotic Fluid and Its ImplicationsDocument4 pagesResearch Article Risk Factors For Meconium Stained Amniotic Fluid and Its ImplicationsAnonymous s8YWSzNo ratings yet