You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Flexin Marketing ReportDocument68 pagesFlexin Marketing ReportHammad BukhariNo ratings yet
- DepakoteDocument5 pagesDepakotejNo ratings yet
- Potpourri of Healing SecretsDocument11 pagesPotpourri of Healing SecretsSamee's Music100% (3)
- Homework A1Document5 pagesHomework A1yellowfish31303No ratings yet
- StrokeDocument9 pagesStrokeezar Al barraqNo ratings yet
- VDVDocument5 pagesVDVVenkatesan VidhyaNo ratings yet
- Aspirin in Episodic Tension-Type Headache: Placebo-Controlled Dose-Ranging Comparison With ParacetamolDocument9 pagesAspirin in Episodic Tension-Type Headache: Placebo-Controlled Dose-Ranging Comparison With ParacetamolErwin Aritama IsmailNo ratings yet
- Laporan Kasus SolDocument32 pagesLaporan Kasus SolameliaNo ratings yet
- Model Paper 4Document22 pagesModel Paper 4Mobin Ur Rehman KhanNo ratings yet
- Formative Test I NBSS 2021-2022 - Attempt ReviewDocument30 pagesFormative Test I NBSS 2021-2022 - Attempt ReviewAlif YusufNo ratings yet
- The Efficacy of Venlafaxine, Flunarizine, and Valproic Acid in The Prophylaxis of Vestibular MigraineDocument5 pagesThe Efficacy of Venlafaxine, Flunarizine, and Valproic Acid in The Prophylaxis of Vestibular MigraineagustianaNo ratings yet
- Nat Prog Book 1 PDFDocument430 pagesNat Prog Book 1 PDFIoana Brăteanu100% (1)
- PANRE and PANCE Review Emergency MedicineDocument15 pagesPANRE and PANCE Review Emergency MedicineThe Physician Assistant Life100% (2)
- Cva 1Document42 pagesCva 1ياسر كوثر هانيNo ratings yet
- Second Partial: Technical University of AmbatoDocument70 pagesSecond Partial: Technical University of AmbatoEdgar MartinezNo ratings yet
- A Brief Materia Medica of Some Lesser-Known NosodesDocument103 pagesA Brief Materia Medica of Some Lesser-Known NosodesnitkolNo ratings yet
- Pyrosid CapsuleDocument3 pagesPyrosid Capsulehk_scribdNo ratings yet
- Herbs and Formulas That Release The ExteriorDocument41 pagesHerbs and Formulas That Release The ExteriorFrancisco VilaróNo ratings yet
- Quick Code ListDocument18 pagesQuick Code Listsjjhala100% (4)
- Medical Record Summary Template (Disability)Document17 pagesMedical Record Summary Template (Disability)Alipit Jr. D. ArmanNo ratings yet
- This Patient Have A Hemorrhagic StrokeDocument7 pagesThis Patient Have A Hemorrhagic StrokeMario ARNo ratings yet
- Neuro 4 - QuestionsDocument50 pagesNeuro 4 - Questionskim100% (1)
- Clinical Case Scenarios Slide Set Powerpoint 2183787181Document58 pagesClinical Case Scenarios Slide Set Powerpoint 2183787181saheefaNo ratings yet
- Headache History TakingDocument6 pagesHeadache History TakingParsaant SinghNo ratings yet
- Mollah MD Foysal - MALE - 21 Yrs +918867572813 AHJN.0000204829 2306447Document3 pagesMollah MD Foysal - MALE - 21 Yrs +918867572813 AHJN.0000204829 2306447Adyan FoysalNo ratings yet
- Talley & O'Connor Quiz SampleDocument5 pagesTalley & O'Connor Quiz SamplefilchibuffNo ratings yet
- MeningiomaDocument7 pagesMeningiomadrhendyjuniorNo ratings yet
- Space Occupying LesionDocument10 pagesSpace Occupying LesionAnna Moser100% (1)
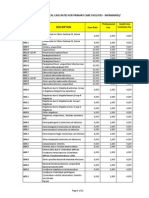
- PhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesDocument22 pagesPhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesChrysanthus HerreraNo ratings yet
- Acupressure Points For Brain StimulationDocument9 pagesAcupressure Points For Brain Stimulationلوليتا وردةNo ratings yet