You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
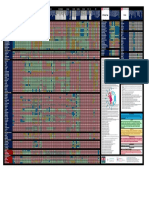
- Antibiotic Cross-Sensitivity ChartDocument1 pageAntibiotic Cross-Sensitivity Chartsuper0113No ratings yet
- Antibiotic Cross-Sensitivity Chart PDFDocument1 pageAntibiotic Cross-Sensitivity Chart PDFanareadsNo ratings yet
- Sanford v2Document1 pageSanford v2sara elalfyNo ratings yet
- EDX Final ProjectDocument2 pagesEDX Final Projectshi_ryuuNo ratings yet
- EDX Final ProjectDocument2 pagesEDX Final Projectshi_ryuuNo ratings yet
- Please State The Name of Your Tutor On The Application Form (Remarks Field)Document1 pagePlease State The Name of Your Tutor On The Application Form (Remarks Field)shi_ryuuNo ratings yet
- Website Usability Final Version August2007Document21 pagesWebsite Usability Final Version August2007Mumtahina MahmudNo ratings yet
- Maurice Nicoll The Mark PDFDocument4 pagesMaurice Nicoll The Mark PDFErwin KroonNo ratings yet
- Form Survailans HAIs Harian OKDocument64 pagesForm Survailans HAIs Harian OKbio rizkimaulanaNo ratings yet
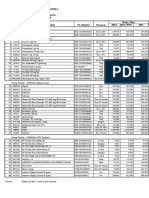
- Stok Obat 6 Sept 18 PDFDocument32 pagesStok Obat 6 Sept 18 PDFMargareta BokaNo ratings yet
- CephalosporinDocument3 pagesCephalosporinbeautifuljade_16No ratings yet
- Daftar Obat High AlertDocument2 pagesDaftar Obat High Alertayu aNo ratings yet
- Antibiotic Cross Sensitivity ChartDocument1 pageAntibiotic Cross Sensitivity Chartthao hoangNo ratings yet
- Cefa DrugsDocument9 pagesCefa DrugsBishan Dutt TiwariNo ratings yet
- 1) Cephalosporins: Generation Common Dosages/Regimens Spectrum of Activity 1 Cephalexin (Keflex) 250-500mg PO q6hDocument1 page1) Cephalosporins: Generation Common Dosages/Regimens Spectrum of Activity 1 Cephalexin (Keflex) 250-500mg PO q6hjoe thomasNo ratings yet
- AntibioticDocument11 pagesAntibioticAmarnath SahNo ratings yet
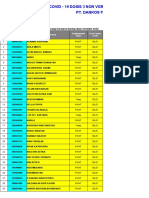
- 2022 - 03 - 12 - Peserta Vaksin Pemerintah Dosis 3 PT. Dankos FarmaDocument31 pages2022 - 03 - 12 - Peserta Vaksin Pemerintah Dosis 3 PT. Dankos FarmaIrsyadNo ratings yet
- List of Cephalosporins + Uses, Types & Side EffectsDocument5 pagesList of Cephalosporins + Uses, Types & Side EffectsMd. Sabit Ahsan SarkerNo ratings yet
- Farmakoloji İlac GruplarıDocument93 pagesFarmakoloji İlac Gruplarıayse100% (1)
- Annexure - Zeiss Pharma TP PDFDocument3 pagesAnnexure - Zeiss Pharma TP PDFPharmaPackaging SolutionsNo ratings yet
- AsoDocument3 pagesAsoKedokteran ShopNo ratings yet
- CephalosporinDocument8 pagesCephalosporinvidagurlNo ratings yet
- Cephalosporins Quick ReviewDocument19 pagesCephalosporins Quick ReviewErinson Custodio PlasenciaNo ratings yet
- CEPHALOSPORINSDocument18 pagesCEPHALOSPORINSVikas SharmaNo ratings yet
- Antibiotik Dan Triamcinolon IntravitrealDocument17 pagesAntibiotik Dan Triamcinolon IntravitrealMeironiWaimirNo ratings yet
- Input FakturDocument477 pagesInput FakturditaNo ratings yet
- Cephalosporin Manufacturers IndiaDocument108 pagesCephalosporin Manufacturers IndiaSingh PushpanjaliNo ratings yet
- Cephalosporins Andes Craig PDFDocument18 pagesCephalosporins Andes Craig PDFMansi singhNo ratings yet
- Data Sales Bulan September 2020Document12 pagesData Sales Bulan September 2020Sujatmiko GintingNo ratings yet
- Data Pembelian September 2016Document12 pagesData Pembelian September 2016Uus HarryNo ratings yet
- Cephalosporins in Animals - DosagesDocument7 pagesCephalosporins in Animals - DosagesSunilNo ratings yet
- Pt. Merapi Utama Pharma Daftar Harga Prinsipal: PT. Meiji Indonesia Berlaku: 23 Oktober 2020Document3 pagesPt. Merapi Utama Pharma Daftar Harga Prinsipal: PT. Meiji Indonesia Berlaku: 23 Oktober 2020AtmaNo ratings yet
- Price List With Net RateDocument1 pagePrice List With Net RateRana TayyabNo ratings yet
- Farmakologi Jilid 2Document158 pagesFarmakologi Jilid 2TeguhsadjadNo ratings yet
- SS-Laktamski Antibiotici: Peroralni Parenteralni Penicilaza Rezistentni PeniciliniDocument5 pagesSS-Laktamski Antibiotici: Peroralni Parenteralni Penicilaza Rezistentni PeniciliniMali PrstNo ratings yet