You might also like
- Gastroenteritis PDFDocument5 pagesGastroenteritis PDFLikhna PertiwiNo ratings yet
- 02 CSB TextDocument143 pages02 CSB TextAnil PanditNo ratings yet
- Eco Criticism and ConsilienceDocument10 pagesEco Criticism and ConsilienceAnil PanditNo ratings yet
- Puffed-Cheek CT Improves Evaluation of The Oral CavityDocument4 pagesPuffed-Cheek CT Improves Evaluation of The Oral CavityAnil PanditNo ratings yet
- Password Net SGIMSDocument1 pagePassword Net SGIMSAnil PanditNo ratings yet
- Book1 Recovered)Document2 pagesBook1 Recovered)Anil PanditNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DRUG STUDY CefuroximeDocument2 pagesDRUG STUDY CefuroximeParado Cabañal Skyliegh50% (2)
- Tugas Individu Skrining: TP TP+ FN TN TN+ FPDocument3 pagesTugas Individu Skrining: TP TP+ FN TN TN+ FPAnonymusNo ratings yet
- Effectiveness of Planned Teaching Programme On Knowledge Regarding Needle Stick Injury Among The Staff NursesDocument3 pagesEffectiveness of Planned Teaching Programme On Knowledge Regarding Needle Stick Injury Among The Staff NursesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Drinking Water AssignmentDocument2 pagesDrinking Water Assignmentpraveenpedagandham100% (1)
- Hospital Administration: Dr. Jayesh PatidarDocument51 pagesHospital Administration: Dr. Jayesh PatidarBraj BhushanNo ratings yet
- Essay HivDocument2 pagesEssay HivPopoo KyoNo ratings yet
- Occupational DiseaseDocument6 pagesOccupational DiseaseBhupesh KumarNo ratings yet
- Pre Employment Health AssessmentDocument7 pagesPre Employment Health AssessmentMP13No ratings yet
- Dennis BurtonDocument1 pageDennis Burtonapoorva_mandavilliNo ratings yet
- Quiz No 3 Tle 10Document2 pagesQuiz No 3 Tle 10Israel Marquez100% (1)
- ESHP Manual Set 1Document3 pagesESHP Manual Set 1Ge Villaver-SalvaneNo ratings yet
- CHECKLIST PROCEDURES (Immunization)Document3 pagesCHECKLIST PROCEDURES (Immunization)Elaine Frances IlloNo ratings yet
- Ending The StigmaDocument1 pageEnding The StigmaarielNo ratings yet
- GMPSADocument6 pagesGMPSAJames TingNo ratings yet
- Brief History of Midwifery in PhilippinesDocument3 pagesBrief History of Midwifery in PhilippinesDivina Gracia Vibal Cielo67% (3)
- Activity-5 2Document4 pagesActivity-5 2Kate MendozaNo ratings yet
- Risk Assessment Form-DECADocument3 pagesRisk Assessment Form-DECAHill CordialNo ratings yet
- Relative Risk and Absolute Risk ReductionDocument4 pagesRelative Risk and Absolute Risk ReductionMatthew Lei0% (1)
- Problem-Based Learning (PBL)Document8 pagesProblem-Based Learning (PBL)dearly reantilloNo ratings yet
- IFRC PHAST Baseline SurveyDocument8 pagesIFRC PHAST Baseline Surveydesign salamNo ratings yet
- School Nurses ' Perspectives On The Role of The School Nurse in Health Education and Health Promotion in England: A Qualitative StudyDocument9 pagesSchool Nurses ' Perspectives On The Role of The School Nurse in Health Education and Health Promotion in England: A Qualitative StudyBarrak AldosaryNo ratings yet
- CVX Length SOGCDocument14 pagesCVX Length SOGCBrendaNo ratings yet
- Session 2 - Sufficient Causes ModelDocument51 pagesSession 2 - Sufficient Causes Modelfrank kipkoechNo ratings yet
- Our Big ContradictionDocument1 pageOur Big ContradictionFerran PibernatNo ratings yet
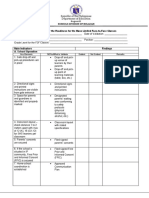
- Checklist For The Readiness For The Mass Limited Face To Face ClassesDocument6 pagesChecklist For The Readiness For The Mass Limited Face To Face Classeschristine jumaquioNo ratings yet
- Annotated BibliographyDocument8 pagesAnnotated BibliographyAmanda CookNo ratings yet
- Emerging and Re Emerging DiseasesDocument49 pagesEmerging and Re Emerging DiseasesteklayNo ratings yet
- Viral Hepatitis in Pregnancy: DR Eleni Nastouli Consultant in Virology and Paediatric Infectious DiseasesDocument34 pagesViral Hepatitis in Pregnancy: DR Eleni Nastouli Consultant in Virology and Paediatric Infectious Diseasesrilla saeliputriNo ratings yet
- Jom Sertai Cep Online TrainingDocument4 pagesJom Sertai Cep Online TrainingDerick ChiaNo ratings yet