You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- TBM Operation For Tunneling Work (Final) PDFDocument117 pagesTBM Operation For Tunneling Work (Final) PDFkiller_pro75% (8)
- AtlesDocument26 pagesAtlesAnonymous CdUZMZJq73No ratings yet
- Airo Part ManualDocument52 pagesAiro Part ManualCemYurtseverNo ratings yet
- Project Report On Pavement DesignDocument50 pagesProject Report On Pavement Designsagar kumar100% (1)
- TransChicago Truck Group Project SummaryDocument17 pagesTransChicago Truck Group Project SummaryTodd FeurerNo ratings yet
- Spare Parts Catalogue: Bajaj Auto LimitedDocument46 pagesSpare Parts Catalogue: Bajaj Auto LimitedGabriel ZamoraNo ratings yet
- FraseologiaDocument52 pagesFraseologiaBruno GanicocheNo ratings yet
- NahDocument3 pagesNahmico de jesusNo ratings yet
- Engineer Estimate ManualDocument24 pagesEngineer Estimate ManualNes-tValdezNo ratings yet
- BS en 45545-5-2013Document20 pagesBS en 45545-5-2013Shiv PandeyNo ratings yet
- Topic 3: Ship's Stresses: MTR 1102 - Ship, Ship Routines and Ship ConstructionDocument25 pagesTopic 3: Ship's Stresses: MTR 1102 - Ship, Ship Routines and Ship ConstructionJuan GonzalesNo ratings yet
- Asu Skysong Map and DirectionsDocument3 pagesAsu Skysong Map and DirectionsCarleone PrimaNo ratings yet
- Indian Biogas Association Biogas Market IndiaDocument36 pagesIndian Biogas Association Biogas Market Indiasj singh100% (1)
- What Does Fedex Deliver?Document17 pagesWhat Does Fedex Deliver?duckythiefNo ratings yet
- HSC Engineering StudiesDocument13 pagesHSC Engineering StudiesRick ThuranNo ratings yet
- Cessna 404Document11 pagesCessna 404AnkkyloFGNo ratings yet
- 5l - FORMDocument7 pages5l - FORMAnthony Steve LomilloNo ratings yet
- Gaz Classifieds 150514Document5 pagesGaz Classifieds 150514Digital MediaNo ratings yet
- Soal UTS 1-1Document2 pagesSoal UTS 1-1Fitri AnnaNo ratings yet
- Highwaymaintenance M KennyDocument28 pagesHighwaymaintenance M KennyEbsa KelifaNo ratings yet
- National Crane NBT40: Operator ManualDocument128 pagesNational Crane NBT40: Operator ManualAlex Sandro Borges Pereira100% (1)
- Legislative Decree 271 - 99Document14 pagesLegislative Decree 271 - 99volgNo ratings yet
- Specific Poa - TX Blank FormDocument1 pageSpecific Poa - TX Blank FormTyler BealsNo ratings yet
- Participating Stations Sep 2020 PDFDocument3 pagesParticipating Stations Sep 2020 PDFمحمد ﺫﻭﻟﻔﮑﺮ محمد بصيNo ratings yet
- Gas DesighDocument81 pagesGas DesighNetra Nanda100% (1)
- 2006 5 Citroen c4 63714 PDFDocument218 pages2006 5 Citroen c4 63714 PDFMuhammad ShahidNo ratings yet
- New Insignia Prices FRDocument24 pagesNew Insignia Prices FRNikos Anta TagalhsNo ratings yet
- Svenborg Disc BrakesDocument112 pagesSvenborg Disc BrakesvsarrNo ratings yet
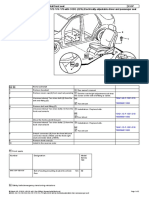
- R&I Seat Belt Buckle Front #2Document2 pagesR&I Seat Belt Buckle Front #2Pablo LoboNo ratings yet