You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- CUT: A Guide To AdulterantsDocument59 pagesCUT: A Guide To AdulterantsVanessa Nicole85% (13)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
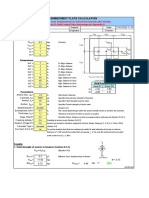
- Embedded Plates Calculation - Part 2Document8 pagesEmbedded Plates Calculation - Part 2Mai CNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Couple of Minutes LaterDocument10 pagesA Couple of Minutes LaterNavi Rai33% (3)
- Contract Termination AgreementDocument3 pagesContract Termination AgreementMohamed El Abany0% (1)
- FM 2-91.4 2008 Intelligence Support To Urban OperationsDocument154 pagesFM 2-91.4 2008 Intelligence Support To Urban OperationsBruce JollyNo ratings yet
- Home Alone 2Document2 pagesHome Alone 2elle maxNo ratings yet
- History of IlokanoDocument8 pagesHistory of IlokanoZoilo Grente Telagen100% (3)
- People's Trans East v. Doctors of New MillenniumDocument3 pagesPeople's Trans East v. Doctors of New MillenniumJayson RacalNo ratings yet
- Delpher Trades Corp v. IAC DigestDocument3 pagesDelpher Trades Corp v. IAC DigestAbigayle Recio100% (1)
- In Re Cunanan 94 PHIL. 534, MARCH 18, 1954 FactsDocument2 pagesIn Re Cunanan 94 PHIL. 534, MARCH 18, 1954 FactsMagr EscaNo ratings yet
- Opioid Conversion ChartDocument4 pagesOpioid Conversion ChartVanessa NicoleNo ratings yet
- Trans Dermal Fentanyl PatchesDocument9 pagesTrans Dermal Fentanyl PatchesVanessa NicoleNo ratings yet
- Meter HandoutDocument8 pagesMeter HandoutudayanilNo ratings yet
- Lesson Free Speech Internet-2Document11 pagesLesson Free Speech Internet-2Paula De Sousa-MouroNo ratings yet
- Income Tax (Deduction For Expenses in Relation To Secretarial Fee and Tax Filing Fee) Rules 2014 (P.U. (A) 336-2014)Document1 pageIncome Tax (Deduction For Expenses in Relation To Secretarial Fee and Tax Filing Fee) Rules 2014 (P.U. (A) 336-2014)Teh Chu LeongNo ratings yet
- G.R. No. L-1477 January 18, 1950 THE PEOPLE OF THE PHILIPPINES, Plaintiff-Appellee, JULIO GUILLEN, Defendant-AppellantDocument8 pagesG.R. No. L-1477 January 18, 1950 THE PEOPLE OF THE PHILIPPINES, Plaintiff-Appellee, JULIO GUILLEN, Defendant-AppellantAnsherina FranciscoNo ratings yet
- Significance of Black History MonthDocument6 pagesSignificance of Black History MonthRedemptah Mutheu MutuaNo ratings yet
- CAT Model FormDocument7 pagesCAT Model FormSivaji Varkala100% (1)
- (20100401) Stryker Spin Boldak Report MinDocument90 pages(20100401) Stryker Spin Boldak Report MinNoel Jameel AbdullahNo ratings yet
- How Did The Various Events in Jose RizalDocument1 pageHow Did The Various Events in Jose RizalErika Joyce Dela CruzNo ratings yet
- Section 19 of HMA ActDocument2 pagesSection 19 of HMA ActNandini SaikiaNo ratings yet
- John Petsche IndictmentDocument2 pagesJohn Petsche IndictmentWKYC.comNo ratings yet
- AML Assignment 2Document6 pagesAML Assignment 2Viraj JoshiNo ratings yet
- 3-Iqbal's Political Philosophy KishwarDocument14 pages3-Iqbal's Political Philosophy KishwarAisha KhatibiNo ratings yet
- Consti 2 Syllabus 2021Document17 pagesConsti 2 Syllabus 2021Cookie MasterNo ratings yet
- Partnership PRE-MID PersonalDocument12 pagesPartnership PRE-MID PersonalAbigail LicayanNo ratings yet
- Ripple ComplaintDocument4 pagesRipple ComplaintLaw&CrimeNo ratings yet
- Europe in The Contemporary World PDFDocument2 pagesEurope in The Contemporary World PDFKellyNo ratings yet
- Objectives: by The End of This Lesson, We WillDocument17 pagesObjectives: by The End of This Lesson, We WillAlyssa Coleen Patacsil DoloritoNo ratings yet
- Star Paper Corporation vs. Simbol 487 SCRA 228 G.R. No. 164774 April 12 2006Document13 pagesStar Paper Corporation vs. Simbol 487 SCRA 228 G.R. No. 164774 April 12 2006Angelie FloresNo ratings yet
- United States v. Daniel J. Driscoll, 399 F.2d 135, 2d Cir. (1968)Document10 pagesUnited States v. Daniel J. Driscoll, 399 F.2d 135, 2d Cir. (1968)Scribd Government DocsNo ratings yet
- Transpo Case ReportDocument10 pagesTranspo Case ReportJesse AlindoganNo ratings yet
- 1038Document34 pages1038Beis MoshiachNo ratings yet
- Central Azucarera de Tarlac G.R. No. 188949Document8 pagesCentral Azucarera de Tarlac G.R. No. 188949froilanrocasNo ratings yet