You might also like
- VQ Ratio in Ards FisiologiDocument21 pagesVQ Ratio in Ards FisiologiSamuel Hananiel RoryNo ratings yet
- Dafpus Ror BDHDocument3 pagesDafpus Ror BDHSamuel Hananiel RoryNo ratings yet
- Board Chronic Pain ManagementDocument1 pageBoard Chronic Pain ManagementSamuel Hananiel RoryNo ratings yet
- Board Opioid Agonist and AntagonistDocument5 pagesBoard Opioid Agonist and AntagonistSamuel Hananiel RoryNo ratings yet
- SamataDocument1 pageSamataSamuel Hananiel RoryNo ratings yet
- Board Airway ManagementDocument2 pagesBoard Airway ManagementSamuel Hananiel RoryNo ratings yet
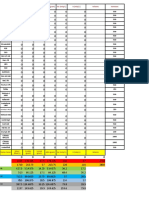
- Nama Cairan KBH (Gram) Na (Meq/L) K (Meq/L) Kemasan Kalori (Kkal/L) Protein (Gram) Lemak (Gram)Document2 pagesNama Cairan KBH (Gram) Na (Meq/L) K (Meq/L) Kemasan Kalori (Kkal/L) Protein (Gram) Lemak (Gram)Samuel Hananiel RoryNo ratings yet
- Board Anesthesia For Patient With Neuropsychiatric DiseaseDocument2 pagesBoard Anesthesia For Patient With Neuropsychiatric DiseaseSamuel Hananiel RoryNo ratings yet
- Spinal, Epidural, Caudal Blocks Postdural Puncture Headache (PDPH)Document2 pagesSpinal, Epidural, Caudal Blocks Postdural Puncture Headache (PDPH)Samuel Hananiel RoryNo ratings yet
- 6320 12312 2 PBDocument8 pages6320 12312 2 PBJhun EjuNo ratings yet
- AnalgesikDocument3 pagesAnalgesikSamuel Hananiel RoryNo ratings yet
- Challenging Because Elderly Patients Are Usually Associated With Severe Cardiovascular ComorbiditiesDocument2 pagesChallenging Because Elderly Patients Are Usually Associated With Severe Cardiovascular ComorbiditiesSamuel Hananiel RoryNo ratings yet
- Traumatic Brain InjuryDocument14 pagesTraumatic Brain InjurySamuel Hananiel RoryNo ratings yet
- Catatan Res AloDocument9 pagesCatatan Res AloSamuel Hananiel RoryNo ratings yet
- Catatan Res AloDocument9 pagesCatatan Res AloSamuel Hananiel RoryNo ratings yet
- Traumatic Brain InjuryDocument14 pagesTraumatic Brain InjurySamuel Hananiel RoryNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Care of High Risk Newborn - ChaboyDocument9 pagesCare of High Risk Newborn - Chaboychfalguera0% (1)
- APTA Combined Sections Meeting 2008: Fugl-Meyer AssessmentDocument17 pagesAPTA Combined Sections Meeting 2008: Fugl-Meyer AssessmentDaniele Bertolo100% (1)
- Denumire Comerciala DCI Forma Farmaceutica ConcentratieDocument4 pagesDenumire Comerciala DCI Forma Farmaceutica ConcentratieAlina CiugureanuNo ratings yet
- Breast LumpDocument2 pagesBreast Lumplentini@maltanet.netNo ratings yet
- Social Anxiety Disorder: Clinical PracticeDocument10 pagesSocial Anxiety Disorder: Clinical PracticeMarcelo Falcão BarrosNo ratings yet
- 2nd Brochure PDFDocument2 pages2nd Brochure PDFhappy855No ratings yet
- Herbal Drugs Standardization ReviewDocument14 pagesHerbal Drugs Standardization ReviewAhmad Daud OmNo ratings yet
- OT AssistantDocument9 pagesOT AssistantIshfaq LoneNo ratings yet
- House-Tree-Person Projective Technique A Validation of Its Use in Occupational TherapyDocument11 pagesHouse-Tree-Person Projective Technique A Validation of Its Use in Occupational Therapyrspecu100% (1)
- Daftar Obat High AlertDocument2 pagesDaftar Obat High Alertayu aNo ratings yet
- Joint Disorders - Ay NewDocument46 pagesJoint Disorders - Ay NewPraisingson SyiemliehNo ratings yet
- Chapter33Walker2015 PDFDocument12 pagesChapter33Walker2015 PDFMai AngelNo ratings yet
- BLS Adult Skills Checklist 2016Document2 pagesBLS Adult Skills Checklist 2016Wahyudi QorahmanNo ratings yet
- Five Element PointsDocument42 pagesFive Element PointsSundar Rajan78% (9)
- R3 Vital Pulp Therapy With New MaterialsDocument7 pagesR3 Vital Pulp Therapy With New MaterialsWening TyasNo ratings yet
- GupisoneDocument7 pagesGupisoneahibba.03862No ratings yet
- List of Empanelled Hospitals/Diagnostic Centres, and Cghs RatesDocument53 pagesList of Empanelled Hospitals/Diagnostic Centres, and Cghs RatesArputNo ratings yet
- Damon Torque and Bracket Placement GuideDocument2 pagesDamon Torque and Bracket Placement GuideMarlina Adrini Turnodihardjo57% (7)
- INTERN-3 Community Pharmacy ProfileDocument34 pagesINTERN-3 Community Pharmacy ProfilejadeNo ratings yet
- Home Visit Infection Control ChecklistDocument3 pagesHome Visit Infection Control ChecklistOlaya alghareniNo ratings yet
- Compartment SyndromeDocument29 pagesCompartment SyndromeFazmial UjirNo ratings yet
- Toxicology Procedures ManualDocument227 pagesToxicology Procedures ManualBenjel AndayaNo ratings yet
- Ejercicios DBT (TDC)Document4 pagesEjercicios DBT (TDC)vanessa_lm_No ratings yet
- Retainer types and uses in orthodonticsDocument6 pagesRetainer types and uses in orthodonticsSahana RangarajanNo ratings yet
- HysterectomyDocument25 pagesHysterectomyCreighton A. BayonganNo ratings yet
- Cut Sheet GE Infinia HawkeyeDocument2 pagesCut Sheet GE Infinia HawkeyeselvamejiaNo ratings yet
- Ramadan NutritionDocument27 pagesRamadan NutritionselcankhatunNo ratings yet
- Triage in Medicine PDFDocument13 pagesTriage in Medicine PDFElsya ApriliaNo ratings yet
- 1 s2.0 S0022391302002998 MainDocument5 pages1 s2.0 S0022391302002998 MainManjeev GuragainNo ratings yet
- 6 Vol. 7 Issue 9 September 2016 IJPSR RE 1915Document9 pages6 Vol. 7 Issue 9 September 2016 IJPSR RE 1915Nur KhasanahNo ratings yet