You might also like
- Diabetes PresentationDocument32 pagesDiabetes PresentationsgolbariNo ratings yet
- Dysfunction of The Endocrine Pancreas:: Diabetes MellitusDocument27 pagesDysfunction of The Endocrine Pancreas:: Diabetes Mellitushasan ismaelNo ratings yet
- Module 08 - Endocrine DisordersDocument43 pagesModule 08 - Endocrine DisordersKarina LojaNo ratings yet
- Review Notes For Diabetes MellitusDocument8 pagesReview Notes For Diabetes MellitusEditha LucasNo ratings yet
- Diabetes Millitus PDFDocument41 pagesDiabetes Millitus PDFAbdullah BhattiNo ratings yet
- Proficiency Testbuilder 4th EditionDocument27 pagesProficiency Testbuilder 4th EditionNgan LeNo ratings yet
- Endocrine - PathophysiologyDocument66 pagesEndocrine - Pathophysiologyskeebs23100% (2)
- Diabetes MellitusDocument44 pagesDiabetes MellituslkristinNo ratings yet
- Diabetes MellitusDocument24 pagesDiabetes MellitusIgwe SolomonNo ratings yet
- OMD-4 Diagnosis and Dental Managment of Diabetes Mellitus Lecture HandoutDocument13 pagesOMD-4 Diagnosis and Dental Managment of Diabetes Mellitus Lecture Handouthananalkadi94No ratings yet
- Diabetes Mellitus: - ClassificationDocument22 pagesDiabetes Mellitus: - ClassificationFernando Junior Parra UchasaraNo ratings yet
- Diabetes1Document150 pagesDiabetes1Phyan HyunNo ratings yet
- Diabetes Mellitus: WAHYUDI, S.Farm., AptDocument31 pagesDiabetes Mellitus: WAHYUDI, S.Farm., AptMayesti FransiskaNo ratings yet
- Shaina Dionisia Palacol Candice Guillermo Gelzan RoldanDocument55 pagesShaina Dionisia Palacol Candice Guillermo Gelzan RoldanEdelrose LapitanNo ratings yet
- Diabetes Mellitus: Risks FactorsDocument5 pagesDiabetes Mellitus: Risks FactorsAmer Abdulla SachitNo ratings yet
- Endocrine - DI, DM I & II 04/13/2016: Review of Endocrine Pancreas: Endocrine and Exocrine Gland Alpha CellsDocument6 pagesEndocrine - DI, DM I & II 04/13/2016: Review of Endocrine Pancreas: Endocrine and Exocrine Gland Alpha Cellsapi-314805004No ratings yet
- Module 8 Assessment and Management of Patients With DiabetesDocument44 pagesModule 8 Assessment and Management of Patients With DiabetesBlessed GarcianoNo ratings yet
- Emd166 Slide Acute Complication of DiabetesDocument78 pagesEmd166 Slide Acute Complication of DiabetesSukma WicaturatmashudiNo ratings yet
- Diabetes MellitusDocument18 pagesDiabetes MellitusAadhan ArveeNo ratings yet
- Diabetes ComplicationsDocument29 pagesDiabetes ComplicationsTom ThomasNo ratings yet
- Course Name: Pharmacology Ii Course Code:Shs.314 Credit Hours: 2Hrs Lectures: 20 INSTRUCTOR: Dr. KhurramDocument27 pagesCourse Name: Pharmacology Ii Course Code:Shs.314 Credit Hours: 2Hrs Lectures: 20 INSTRUCTOR: Dr. KhurramAmynah WasimNo ratings yet
- Diabetes Mellitus Complications: Ssenabulya F Ronny MBCHB V Moderator Dr. Mutebi 4B Endocrinology UnitDocument55 pagesDiabetes Mellitus Complications: Ssenabulya F Ronny MBCHB V Moderator Dr. Mutebi 4B Endocrinology UnitNinaNo ratings yet
- Diabetes Mellitus Type2: Case StudyDocument48 pagesDiabetes Mellitus Type2: Case StudyJohn Carlo GarciaNo ratings yet
- Diabetes: InvestigationsDocument8 pagesDiabetes: InvestigationsJason YousafNo ratings yet
- Diabetes Mellitus PatientsDocument33 pagesDiabetes Mellitus PatientsShabeel PnNo ratings yet
- Anesthesia and Diabetes: Marwa Ahmad MahrousDocument79 pagesAnesthesia and Diabetes: Marwa Ahmad MahrousAjengNo ratings yet
- Lecture - Paediatric Endocrine Emergencies PDFDocument51 pagesLecture - Paediatric Endocrine Emergencies PDFOnSolomonNo ratings yet
- Emergencies in Diabetes: R Bowo Pramono Perkeni Cabang YogyakartaDocument31 pagesEmergencies in Diabetes: R Bowo Pramono Perkeni Cabang YogyakartaputrinaraheswariNo ratings yet
- Glucose, Part1Document33 pagesGlucose, Part1SarahNo ratings yet
- Clinical SignificanceDocument31 pagesClinical Significancejav israelNo ratings yet
- Patologi Pankreas Endokrin & AdrenalDocument69 pagesPatologi Pankreas Endokrin & AdrenalSonia Afika AzizaNo ratings yet
- Diabetic KetoacidosisDocument12 pagesDiabetic Ketoacidosispolaris_027No ratings yet
- Causes of Metabolic AcidosisDocument10 pagesCauses of Metabolic AcidosisKimberly Anne SP PadillaNo ratings yet
- Classification: LiverDocument20 pagesClassification: LivertermskipopNo ratings yet
- Diabetes Mellitus: Dr. Sajid Abbas JaffriDocument37 pagesDiabetes Mellitus: Dr. Sajid Abbas JaffriMaham ZarrinNo ratings yet
- DKA To CRFDocument4 pagesDKA To CRFMark Anthony YabresNo ratings yet
- Obesitas Mets DMDocument47 pagesObesitas Mets DMFathimah UswahNo ratings yet
- Blood GlucoseDocument8 pagesBlood Glucoseعبدالرحمن عابدNo ratings yet
- E SystemDocument81 pagesE SystemErsido SamuelNo ratings yet
- Acute. KetoacidosisdocxDocument12 pagesAcute. KetoacidosisdocxShara SampangNo ratings yet
- Diabetes MellitusDocument29 pagesDiabetes MellitusFourthMolar.com100% (1)
- Diabetes For Dentists: DR Jackie Elliott Clinical Lecturer in DiabetesDocument37 pagesDiabetes For Dentists: DR Jackie Elliott Clinical Lecturer in DiabetesKevalChavdaNo ratings yet
- Metabolic Endocrine DiabetesDocument16 pagesMetabolic Endocrine DiabetesPatricia Anne Nicole CuaresmaNo ratings yet
- Diabetes Mellitus: NZ Diploma in Enrolled NursingDocument38 pagesDiabetes Mellitus: NZ Diploma in Enrolled NursingRegina PunNo ratings yet
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいNo ratings yet
- Endocrine Emergencies: Lynn K. Wittwer, MD MPD Clark County EMSDocument37 pagesEndocrine Emergencies: Lynn K. Wittwer, MD MPD Clark County EMSSyahril FauziNo ratings yet
- Diabetes MellitusDocument44 pagesDiabetes MellitusDiahNo ratings yet
- Diabetes MellitusDocument34 pagesDiabetes MellitusKobby AmoahNo ratings yet
- Lec 1Document9 pagesLec 1fbbqbcht6yNo ratings yet
- Curs Studenti StrainiDocument71 pagesCurs Studenti StrainiAlexandru VisanNo ratings yet
- Chapter 4 Carbohydrate DisorderDocument26 pagesChapter 4 Carbohydrate DisorderNida RidzuanNo ratings yet
- Clinical ApplicationDocument14 pagesClinical Applicationthe pharmacistNo ratings yet
- Insulin, Diabetes Oral HypoDocument94 pagesInsulin, Diabetes Oral HypoNagu Kopparapu0% (1)
- Endocrine 160110083024Document65 pagesEndocrine 160110083024Ryan CracknellNo ratings yet
- What Is A Subchorionic HemorrhageDocument4 pagesWhat Is A Subchorionic HemorrhageBudo LataquinNo ratings yet
- Diabetes MellitusDocument66 pagesDiabetes MellitusNatson ZmNo ratings yet
- Diabetic Recipes for One and TwoFrom EverandDiabetic Recipes for One and TwoRating: 3 out of 5 stars3/5 (1)
- Bot 301 eDocument3 pagesBot 301 err5633No ratings yet
- F 1040 EsDocument11 pagesF 1040 EsJohn YenNo ratings yet
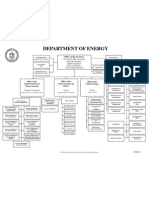
- Doechart-Nonames 2011-12Document1 pageDoechart-Nonames 2011-12rr5633No ratings yet
- Essential Physics 1Document214 pagesEssential Physics 1Zayd Iskandar Dzolkarnain Al-HadramiNo ratings yet
- Tech Guide N8KBR-26pagesDocument27 pagesTech Guide N8KBR-26pagesrr5633No ratings yet
- ECG and ArrhythmiasDocument25 pagesECG and ArrhythmiasRashed ShatnawiNo ratings yet
- Name of Drug Action Indication Contraindication Adverse Reaction Nursing ConsiderationDocument4 pagesName of Drug Action Indication Contraindication Adverse Reaction Nursing ConsiderationClariss AlotaNo ratings yet
- Congenital Nasolacrimal Duct ObstructionDocument43 pagesCongenital Nasolacrimal Duct ObstructionAnumeha JindalNo ratings yet
- Methanol-Induced Optic Nerve Cupping: Photo EssayDocument1 pageMethanol-Induced Optic Nerve Cupping: Photo EssayJose SalgadoNo ratings yet
- Abstract Apicon Category Section Title Author Name Author Name and Contact NumberDocument6 pagesAbstract Apicon Category Section Title Author Name Author Name and Contact NumberKriti KumariNo ratings yet
- Communicable Diseases QuestionsDocument11 pagesCommunicable Diseases QuestionsChelleyOllitro100% (15)
- CPG Management of Cervical Cancer (Second Edition)Document88 pagesCPG Management of Cervical Cancer (Second Edition)ooiziungie100% (1)
- Term Example Discoloration Flat,: Patch ( 1cm) Papule ( 1cm)Document4 pagesTerm Example Discoloration Flat,: Patch ( 1cm) Papule ( 1cm)Almira PutriNo ratings yet
- MRCPass Notes For MRCP 1 - EnDOCRINOLOGYDocument12 pagesMRCPass Notes For MRCP 1 - EnDOCRINOLOGYsabdali100% (1)
- RHB en Cancer, GeneralidadesDocument12 pagesRHB en Cancer, GeneralidadesDaniela Fernanda Cruz GómezNo ratings yet
- Power Point Treatment of Functional Dyspepsia With SertralineDocument26 pagesPower Point Treatment of Functional Dyspepsia With SertralineRadias ZasraNo ratings yet
- Down SyndromeDocument2 pagesDown SyndromeKakoy ZenarosaNo ratings yet
- The Differential Diagnosis of Problematic Hypersexuality: A. J. Reid Finlayson John Sealy Peter R. MartinDocument11 pagesThe Differential Diagnosis of Problematic Hypersexuality: A. J. Reid Finlayson John Sealy Peter R. Martinden777No ratings yet
- QR HypertensionDocument8 pagesQR Hypertensionwaniaqilah workNo ratings yet
- AdhdDocument9 pagesAdhdapi-712048645No ratings yet
- GI Part 2 2016 StudentDocument131 pagesGI Part 2 2016 StudentDaniel RayNo ratings yet
- When Milk Comes Out From Breast What Does That Me PDFDocument1 pageWhen Milk Comes Out From Breast What Does That Me PDFangelo pelleNo ratings yet
- Acute Diarrhea LaDocument38 pagesAcute Diarrhea LaBane LtpNo ratings yet
- Introduction To Infection ControlDocument9 pagesIntroduction To Infection ControlLast YearNo ratings yet
- Jurnal Ilmu Keperawatan Jiwa: Volume 4 Nomor 3, Agustus 2021 e-ISSN 2621-2978 p-ISSN 2685-9394Document10 pagesJurnal Ilmu Keperawatan Jiwa: Volume 4 Nomor 3, Agustus 2021 e-ISSN 2621-2978 p-ISSN 2685-9394ade rina atikahNo ratings yet
- RifampicinDocument2 pagesRifampicinChaeL90No ratings yet
- Nursing Drug Study (Albendazole)Document6 pagesNursing Drug Study (Albendazole)Kristel Diane RidaoNo ratings yet
- PenicillinDocument1 pagePenicillinShaivya Pathak100% (1)
- LENS Skin Disorders 2324Document49 pagesLENS Skin Disorders 2324Zyrille Moira MaddumaNo ratings yet
- TwstrsDocument6 pagesTwstrsahippoNo ratings yet
- Ledderhose Disease: Pathophysiology Diagnosis and ManagementDocument3 pagesLedderhose Disease: Pathophysiology Diagnosis and ManagementLeandro PolancoNo ratings yet
- Distribution and Density of Tertiary Lymphoid Structures Predict Clinical Outcome in Intrahepatic CholangiocarcinomaDocument12 pagesDistribution and Density of Tertiary Lymphoid Structures Predict Clinical Outcome in Intrahepatic Cholangiocarcinoma马三强No ratings yet
- Manual Handling Case Studies Part 1 - Attempt Review PDFDocument30 pagesManual Handling Case Studies Part 1 - Attempt Review PDFMODI KRUNAL100% (2)
- BIOLOGY INVESTIGATORY PROJECT - Cardiovascular Diseases - Coronary Artery Disease PDFDocument50 pagesBIOLOGY INVESTIGATORY PROJECT - Cardiovascular Diseases - Coronary Artery Disease PDFlskumar100% (1)
- Medieval Times ScriptDocument4 pagesMedieval Times Scriptapi-280254861No ratings yet