You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Module 2 Caranay John Lloyd C. NCM 107 BSN 2BDocument6 pagesModule 2 Caranay John Lloyd C. NCM 107 BSN 2BRM MoralesNo ratings yet
- Chapters HarmeetDocument32 pagesChapters HarmeetBlessy MohandassNo ratings yet
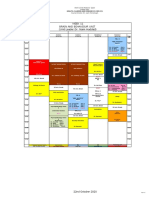
- Week 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)Document1 pageWeek 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)f3er3No ratings yet
- 00 FINAL LPDP Study Plan BrigitaDocument2 pages00 FINAL LPDP Study Plan BrigitaBrigita De VegaNo ratings yet
- 3) Growth of Service SectorDocument9 pages3) Growth of Service SectorAMIN BUHARI ABDUL KHADER100% (1)
- ResumeDocument3 pagesResumeapi-601576828No ratings yet
- Nursamsu B.inggrisDocument2 pagesNursamsu B.inggrisSamsu AnandaNo ratings yet
- FarmasiDocument17 pagesFarmasiI N D INo ratings yet
- Nursing Perspective & JurisprudenceDocument4 pagesNursing Perspective & JurisprudenceRonel-Carmen Nuevo FirmoNo ratings yet
- ForlornDocument4 pagesForlornMeryl OlazoNo ratings yet
- INTERVIEW TO MATRON - Modif.-1Document3 pagesINTERVIEW TO MATRON - Modif.-1Alejandro CastroNo ratings yet
- Nursing Care Plan: Louise O. Reponte BSN-3CDocument12 pagesNursing Care Plan: Louise O. Reponte BSN-3CLouise MurphyNo ratings yet
- Biomedical Engineering: By: Justin Lau, Kaisen Nakagawa, Preston Iha and Nuuanu Tech ClubDocument10 pagesBiomedical Engineering: By: Justin Lau, Kaisen Nakagawa, Preston Iha and Nuuanu Tech ClubS.m. ChandrashekarNo ratings yet
- The Feeling Good Handbook - WikipediaDocument7 pagesThe Feeling Good Handbook - Wikipediacamicris0% (14)
- AABB Billing Guide For Blood Products and Related Services: July 2020 1Document45 pagesAABB Billing Guide For Blood Products and Related Services: July 2020 1Rija KhanNo ratings yet
- Adinda Tri Kurnia Putri - 2011313001 - A32020Document2 pagesAdinda Tri Kurnia Putri - 2011313001 - A32020allvi dayu nengsihNo ratings yet
- Essentials of Medical Laboratory Practice Lieseke Constance L SRGDocument579 pagesEssentials of Medical Laboratory Practice Lieseke Constance L SRGAlexandr TrotskyNo ratings yet
- Occupational English Test Oet Reading Part BC Test 04Document16 pagesOccupational English Test Oet Reading Part BC Test 04AndreaNo ratings yet
- COPD Spirometry ModuleDocument50 pagesCOPD Spirometry ModuleMeydita MahardiNo ratings yet
- CD011145 Pub2Document185 pagesCD011145 Pub2Guilherme RodriguesNo ratings yet
- Spiritual History of NursingDocument59 pagesSpiritual History of NursingVincent Quiña PigaNo ratings yet
- 23011214560126@70 - Pichay, Loren Sta - Teresa - L230000355933 - 2300013461Document2 pages23011214560126@70 - Pichay, Loren Sta - Teresa - L230000355933 - 2300013461maxor4242No ratings yet
- Specialized Industry HospitalDocument55 pagesSpecialized Industry HospitalMelanie SamsonaNo ratings yet
- 109PMC-Effect of A Spiritual Care Program On Levels of Anxiety in Patients With Leukemia-MoeiniDocument7 pages109PMC-Effect of A Spiritual Care Program On Levels of Anxiety in Patients With Leukemia-MoeiniCristina Teixeira PintoNo ratings yet
- Intern Annual16Document7 pagesIntern Annual16Akash PanwarNo ratings yet
- Sanjay Gandhi Post Graduate Institute of Medical Sciences: Raebareli Road, Lucknow - 226 014, IndiaDocument1 pageSanjay Gandhi Post Graduate Institute of Medical Sciences: Raebareli Road, Lucknow - 226 014, IndiaAtul DubeyNo ratings yet
- Britam Medical Service Providers Panel 2022Document219 pagesBritam Medical Service Providers Panel 2022Melissa KhevarliNo ratings yet
- Necrotising Ulcerative Gingivitis: A Literature Review: James Dufty / Nikolaos Gkranias / Nikos DonosDocument10 pagesNecrotising Ulcerative Gingivitis: A Literature Review: James Dufty / Nikolaos Gkranias / Nikos DonosmayaNo ratings yet
- Case Study Dorothea Orem (Francar Jade For Sbmission) - TFNDocument2 pagesCase Study Dorothea Orem (Francar Jade For Sbmission) - TFNFrancar Jade De VeraNo ratings yet
- Critical Care Pharmacy Evolution PDFDocument39 pagesCritical Care Pharmacy Evolution PDFhuong LNo ratings yet