You might also like
- Dirty Sex VocabularyDocument113 pagesDirty Sex Vocabularymichele100% (1)
- The Truth About Female Ejaculation FLODocument18 pagesThe Truth About Female Ejaculation FLORohit NikhalNo ratings yet
- HypersexualityDocument7 pagesHypersexualitysuzyNo ratings yet
- NeurosexologyDocument23 pagesNeurosexologydo2005No ratings yet
- Get Pregnant QuicklyDocument2 pagesGet Pregnant QuicklytmsabarinathanNo ratings yet
- Desire ArousalDocument28 pagesDesire ArousalMuhammad AnwerNo ratings yet
- Sexual Addiction or Hypersexual DisorderDocument9 pagesSexual Addiction or Hypersexual Disorderعلى حسين100% (1)
- The Relationship Between Sexuality, Schizophrenia, And Quality Of LifeFrom EverandThe Relationship Between Sexuality, Schizophrenia, And Quality Of LifeNo ratings yet
- The Female Sexual Function Index FSFI A Multidimensional Self Report Instrument For The Assessment of Female Sexual Function IMPORTANTEDocument19 pagesThe Female Sexual Function Index FSFI A Multidimensional Self Report Instrument For The Assessment of Female Sexual Function IMPORTANTEaperfectcircle7978100% (1)
- The Sexual SelfDocument90 pagesThe Sexual SelfAslia MananNo ratings yet
- Neurobiological Basis of HypersexualityDocument21 pagesNeurobiological Basis of HypersexualityUgur BuyuktezgelNo ratings yet
- Guide To Crazy Good SexDocument9 pagesGuide To Crazy Good SexMbadilishaji DuniaNo ratings yet
- Systemic Rituals in Sexual Therapy by Gary L. SandersDocument17 pagesSystemic Rituals in Sexual Therapy by Gary L. SandersOlena BaevaNo ratings yet
- Development and Validation of The Pretending Orgasm Reasons MeasureDocument19 pagesDevelopment and Validation of The Pretending Orgasm Reasons MeasureEdit Csányi100% (1)
- Porn Studies SlideshowDocument15 pagesPorn Studies Slideshowapi-329029118No ratings yet
- 40 Mistakes Men Make While Having Sex With WomenDocument3 pages40 Mistakes Men Make While Having Sex With WomenJill Camacho100% (2)
- Sex Christian For MenDocument112 pagesSex Christian For Menjb1510100% (2)
- Pharmacology of Sexually Compulsive BehaviorDocument9 pagesPharmacology of Sexually Compulsive Behaviorsara_vonNo ratings yet
- Weight-For-Height BOYS: 2 To 5 Years (Z-Scores)Document1 pageWeight-For-Height BOYS: 2 To 5 Years (Z-Scores)Malisa Lukman100% (1)
- Journal of Sex ResearchDocument10 pagesJournal of Sex ResearchAna Belén AmilNo ratings yet
- The Female Sexual Function Index FSFI A Multidimensional Self Report Instrument For The Assessment of Female Sexual FunctionDocument19 pagesThe Female Sexual Function Index FSFI A Multidimensional Self Report Instrument For The Assessment of Female Sexual FunctionMuhammad ArsalNo ratings yet
- 3.-Func y Disf Sex FemeninaDocument15 pages3.-Func y Disf Sex FemeninaCristina Bravo100% (1)
- Female Sexual Function and Dysfunction - Assessment and Treatment - Obgyn KeyDocument19 pagesFemale Sexual Function and Dysfunction - Assessment and Treatment - Obgyn KeyDorin ScladanNo ratings yet
- Female Homosexual DevelopmentDocument4 pagesFemale Homosexual Developmentpleasure masangoNo ratings yet
- CBT Manual OcdDocument19 pagesCBT Manual OcdRedefining Self with MeghaNo ratings yet
- Sex TherapyDocument18 pagesSex TherapyMonika JosephNo ratings yet
- Rieger (2015) Sexual Arausal in Women - BisexualidadDocument70 pagesRieger (2015) Sexual Arausal in Women - BisexualidadGustavo AyalaNo ratings yet
- Masters and JohnsonDocument5 pagesMasters and JohnsonRuben Poblete50% (2)
- Female Sexual Dysfunction: Classification, Pathophysiology, and ManagementDocument12 pagesFemale Sexual Dysfunction: Classification, Pathophysiology, and ManagementGina Magda RianaNo ratings yet
- Safer Sex GuideDocument4 pagesSafer Sex GuideJuanCarlos YogiNo ratings yet
- MasturbationDocument17 pagesMasturbationRitesh Chandra17% (6)
- tipsPREVIEW2 PDFDocument13 pagestipsPREVIEW2 PDFBaljinder SinghNo ratings yet
- People Vs Bonaagua Crim DigestDocument2 pagesPeople Vs Bonaagua Crim DigestCJ80% (5)
- Female Sexual Dysfunction and The Central Nervous System IIDocument3 pagesFemale Sexual Dysfunction and The Central Nervous System IIAdamNo ratings yet
- Peggy R Lipford McKeal PHD John F Wirth and Melissa Vinson Erotology and The Study of Arousal and DesireDocument64 pagesPeggy R Lipford McKeal PHD John F Wirth and Melissa Vinson Erotology and The Study of Arousal and DesireClaireFitzpatrickNo ratings yet
- Mindfulness-Based Sex Therapy Improves Genital-Subjective Arousal Concordance in Women With Sexual Desire/Arousal DifficultiesDocument15 pagesMindfulness-Based Sex Therapy Improves Genital-Subjective Arousal Concordance in Women With Sexual Desire/Arousal DifficultiesCoteMartinezNo ratings yet
- Sex Therapy 2014Document7 pagesSex Therapy 2014pagoeta012No ratings yet
- FSD Consultation JSM 2017Document56 pagesFSD Consultation JSM 2017dwirabiatul adwiyahaliNo ratings yet
- Portrait of An ExhibitionistDocument15 pagesPortrait of An Exhibitionist116 - Kencana NoorNo ratings yet
- Barlow (1986) Causes of Sexual Dysfunction - The Role of Anxiety and Cognitive InterferenceDocument9 pagesBarlow (1986) Causes of Sexual Dysfunction - The Role of Anxiety and Cognitive InterferenceGloria KentNo ratings yet
- Review: University of The West of Scotland, School of Social Sciences, Paisley, UK DOI: 10.1111/j.1743-6109.2009.01677.xDocument26 pagesReview: University of The West of Scotland, School of Social Sciences, Paisley, UK DOI: 10.1111/j.1743-6109.2009.01677.xRodel CamposoNo ratings yet
- Erika JournalDocument9 pagesErika JournalFariseilaa PurakbarNo ratings yet
- Sexual DysfunctionDocument9 pagesSexual DysfunctionerlandNo ratings yet
- Ocitocina e LibidoDocument10 pagesOcitocina e LibidoFê VidapaleoNo ratings yet
- Experimental PaperDocument11 pagesExperimental Paperapi-642844062No ratings yet
- How Does Premature Ejaculation Impact A Man S LifeDocument11 pagesHow Does Premature Ejaculation Impact A Man S LifeSubham TalukdarNo ratings yet
- JRJRJRJDocument7 pagesJRJRJRJlionfairwayNo ratings yet
- Incomplete Sex-Reassignment Surgery and Psychosocial Functioning: A Preliminary StudyDocument22 pagesIncomplete Sex-Reassignment Surgery and Psychosocial Functioning: A Preliminary StudyPrachi RoutNo ratings yet
- Dusenbury 2017Document13 pagesDusenbury 2017pokharelriwaj82No ratings yet
- DiLillo (2001)Document24 pagesDiLillo (2001)voooNo ratings yet
- Classification and Definition of Premature Ejaculation: Arie Parnham, Ege Can SerefogluDocument8 pagesClassification and Definition of Premature Ejaculation: Arie Parnham, Ege Can SerefogluWanly SyahrizalNo ratings yet
- Female Orgasm and Overall Sexual Function and HabitsDocument11 pagesFemale Orgasm and Overall Sexual Function and HabitsceydaalyazhotamisNo ratings yet
- Jba 04 037Document8 pagesJba 04 037Anno NymousNo ratings yet
- FaisandierDocument11 pagesFaisandierCelesIngaOrtizNo ratings yet
- Physiology of Womens Sexual Function BasDocument24 pagesPhysiology of Womens Sexual Function BasкостяNo ratings yet
- Chivers Seto Blanchard 2007Document14 pagesChivers Seto Blanchard 2007api-292904275No ratings yet
- Maternal Nursing Care - CHPT 6 Human Sexuality and FertilityDocument28 pagesMaternal Nursing Care - CHPT 6 Human Sexuality and Fertilitythubtendrolma100% (1)
- Continuing Medical Education: Sexual Orientation Matters in Sexual MedicineDocument13 pagesContinuing Medical Education: Sexual Orientation Matters in Sexual MedicineAbigailNo ratings yet
- Psychology of Women Quarterly - A Decade of Feminist Influence On Psychotherapy - BrodskyDocument14 pagesPsychology of Women Quarterly - A Decade of Feminist Influence On Psychotherapy - BrodskyKate DevineNo ratings yet
- Sex Therapy 2014Document7 pagesSex Therapy 2014Shuaib AkhterNo ratings yet
- HelgesonLepore SR 1997Document17 pagesHelgesonLepore SR 1997racheldent2000No ratings yet
- The Relationship Between Overactive Bladder and Sexual Activity in WomenDocument11 pagesThe Relationship Between Overactive Bladder and Sexual Activity in WomenJimmy GillNo ratings yet
- What Research Shows: NARTH's Response To The APA Claims On HomosexualityDocument4 pagesWhat Research Shows: NARTH's Response To The APA Claims On Homosexualitybmx0No ratings yet
- Our Data Showed That Sexual Disorders Were Highly PrevalentDocument5 pagesOur Data Showed That Sexual Disorders Were Highly Prevalentsheirly100% (1)
- A Sexual Adjustment Questionnaire For Use in Therapy andDocument10 pagesA Sexual Adjustment Questionnaire For Use in Therapy andVida Y SaludNo ratings yet
- Health-Related Lifestyle Factors and Sexual Dysfunction: A Meta-Analysis of Population-Based ResearchDocument18 pagesHealth-Related Lifestyle Factors and Sexual Dysfunction: A Meta-Analysis of Population-Based ResearchGabino CoronaNo ratings yet
- Feminism & Psychology 2013 Duschinsky 49 55Document8 pagesFeminism & Psychology 2013 Duschinsky 49 55ruth12345678No ratings yet
- Premature Ejaculation Among Chinese Urban Men Prevalence and CorrelatesDocument11 pagesPremature Ejaculation Among Chinese Urban Men Prevalence and CorrelatesZhewen TangNo ratings yet
- Mendez-Shapira2013 Article HypersexualBehaviorInFrontotemDocument9 pagesMendez-Shapira2013 Article HypersexualBehaviorInFrontotemYulesalazarmNo ratings yet
- Gone But Not Forgotten Virginity Loss and Current Sexual SatisfactionDocument17 pagesGone But Not Forgotten Virginity Loss and Current Sexual SatisfactionprastiyowillyNo ratings yet
- Female Sexual DysfunctionDocument17 pagesFemale Sexual Dysfunctionnarayani17No ratings yet
- Burnout in Women Physicians: Prevention, Treatment, and ManagementFrom EverandBurnout in Women Physicians: Prevention, Treatment, and ManagementCynthia M. StonningtonNo ratings yet
- Girls Chart Weight For Length Height Birth To 5 Years (Z Scores)Document1 pageGirls Chart Weight For Length Height Birth To 5 Years (Z Scores)Arie FalahNo ratings yet
- Eclinicalmedicine: Contents Lists Available atDocument9 pagesEclinicalmedicine: Contents Lists Available atArie FalahNo ratings yet
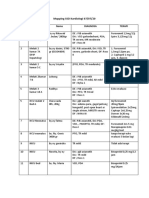
- Mapping SSD Kardiologi 07Document2 pagesMapping SSD Kardiologi 07Arie FalahNo ratings yet
- Arrahman'Document8 pagesArrahman'Arie FalahNo ratings yet
- Mapping SSD Kardiologi 03Document2 pagesMapping SSD Kardiologi 03Arie FalahNo ratings yet
- Parental Depression, Maternal Antidepressant Use During Pregnancy, and Risk of Autism Spectrum Disorders - Population Based Case-Control StudyDocument15 pagesParental Depression, Maternal Antidepressant Use During Pregnancy, and Risk of Autism Spectrum Disorders - Population Based Case-Control StudykajurebaNo ratings yet
- ONELINE PC GAME LIST 27-Oct-2014 - (WWW - Onelinepcgame.com)Document248 pagesONELINE PC GAME LIST 27-Oct-2014 - (WWW - Onelinepcgame.com)Arie FalahNo ratings yet
- Knowledge On Acne Vulgaris and Menstrual Cycle: A Study On Adolescent GirlsDocument8 pagesKnowledge On Acne Vulgaris and Menstrual Cycle: A Study On Adolescent GirlsChristina WiyaniputriNo ratings yet
- 767 FTPDocument5 pages767 FTPArie FalahNo ratings yet
- Raloxifene N OsteoporosisDocument8 pagesRaloxifene N OsteoporosisArie FalahNo ratings yet
- Book 1Document3 pagesBook 1Arie FalahNo ratings yet
- Password 11-11-11Document1 pagePassword 11-11-11Arie FalahNo ratings yet
- Hands Free Automatic Male Masturbator Sucking CupDocument10 pagesHands Free Automatic Male Masturbator Sucking CupNancy WalkerNo ratings yet
- Echoes Article - Tackling The TabooDocument2 pagesEchoes Article - Tackling The TabooFlora Anne R. PalabricaNo ratings yet
- Report-Aravani Sex Work ChennaiDocument22 pagesReport-Aravani Sex Work ChennaibarathyshanmugamNo ratings yet
- Screenshot 2020-11-18 at 5.35.01 PMDocument1 pageScreenshot 2020-11-18 at 5.35.01 PMRose FreakNo ratings yet
- Teenage Sex Should Require Parental ConsentDocument2 pagesTeenage Sex Should Require Parental ConsentAivan LantapeNo ratings yet
- Lesson PlanDocument8 pagesLesson Planapi-314850456No ratings yet
- Sensate Focus EjerciciosDocument2 pagesSensate Focus EjerciciosMarcelo Da Silva0% (1)
- Sissy 1Document3 pagesSissy 1Trixy tangNo ratings yet
- Natasha Nice Cumshot. Top Adult FREE Pic. Comments 1 2Document1 pageNatasha Nice Cumshot. Top Adult FREE Pic. Comments 1 2stellamabel58No ratings yet
- Approaching Sexual Potential in RelationshipDocument13 pagesApproaching Sexual Potential in RelationshipAna AchimNo ratings yet
- LGBTQ PresentationDocument6 pagesLGBTQ PresentationMichaela OlinNo ratings yet
- Sexual Response CycleDocument7 pagesSexual Response CycleHana-Lou TaquiquiNo ratings yet
- Revised ResearchDocument14 pagesRevised ResearchAlynna ValbuenaNo ratings yet
- What Are The Phases of The Sexual Response CycleDocument3 pagesWhat Are The Phases of The Sexual Response CycleLili PangitNo ratings yet
- Haru Nnm's Gay Porn Videos PornhubDocument1 pageHaru Nnm's Gay Porn Videos PornhubchristianabarumeNo ratings yet
- A Position Paper About "Giving Condoms To High School Student"Document2 pagesA Position Paper About "Giving Condoms To High School Student"Cristine Joy Remerata Villarosa93% (14)
- TSH The Sexuality Wheel Tool EnglishDocument2 pagesTSH The Sexuality Wheel Tool EnglishRita TorresNo ratings yet
- What Is Sexual ContinenceDocument2 pagesWhat Is Sexual ContinenceBarbatul Viril PotentNo ratings yet