You might also like
- WHO 2013 PPH HighlightsDocument4 pagesWHO 2013 PPH HighlightsNimeJi B'leaf 윤 재No ratings yet
- J Clin Pathol 2004 Hanley 1132 9Document9 pagesJ Clin Pathol 2004 Hanley 1132 9NimeJi B'leaf 윤 재No ratings yet
- Ice RegimenDocument6 pagesIce RegimenNimeJi B'leaf 윤 재No ratings yet
- Pharmacology and Management of The Vitamin K Antagonists-Chest GuidelineDocument41 pagesPharmacology and Management of The Vitamin K Antagonists-Chest GuidelineNimeJi B'leaf 윤 재No ratings yet
- Ó Springer Science+Business Media, LLC 2008: WWW - Clinicaltrials.govDocument6 pagesÓ Springer Science+Business Media, LLC 2008: WWW - Clinicaltrials.govNimeJi B'leaf 윤 재No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GM Arctic Apple Traits and Approval ProcessDocument12 pagesGM Arctic Apple Traits and Approval ProcessTheresa Paula Dela RosaNo ratings yet
- NB 2023 05 30 05Document15 pagesNB 2023 05 30 05प्रीतम सिंह तोमरNo ratings yet
- Cloning VectorsDocument19 pagesCloning VectorsvmshanesNo ratings yet
- Case Studies of Industrial Biotechnology in The Chemistry-Using Industries PDFDocument20 pagesCase Studies of Industrial Biotechnology in The Chemistry-Using Industries PDFNicole Danielle MallariNo ratings yet
- Microbial Production of Scleroglucan and DSPDocument19 pagesMicrobial Production of Scleroglucan and DSPgandurikNo ratings yet
- NIT WARANGAL PhdbrochureDocument17 pagesNIT WARANGAL Phdbrochurevss swamyNo ratings yet
- Microbiology-Lab Practical SOP - 10Document2 pagesMicrobiology-Lab Practical SOP - 10Biswanath Bhunia100% (1)
- Concise Encyclopedia of Temperate Tree Fruit Singha BasraDocument389 pagesConcise Encyclopedia of Temperate Tree Fruit Singha Basratibi_pl2005100% (6)
- Fmicb 10 00053Document23 pagesFmicb 10 00053hafniomonNo ratings yet
- Fungi, The Good, The Bad and The UglyDocument26 pagesFungi, The Good, The Bad and The UglyMrGilmartinNo ratings yet
- Indian PharmaDocument32 pagesIndian PharmaNidhiNo ratings yet
- Seminars in Orthodontics 2005 CarlsonDocument12 pagesSeminars in Orthodontics 2005 CarlsonMariana Levy100% (1)
- Microbial Identification Methods for Pharmaceutical TestingDocument11 pagesMicrobial Identification Methods for Pharmaceutical TestingSurendar KesavanNo ratings yet
- Top 50 Biotech Companies in IndiaDocument12 pagesTop 50 Biotech Companies in IndiaSumit Kumar Gupta80% (5)
- Bio-Biomedical Graduate Programs Dropping GRE RequirementDocument2 pagesBio-Biomedical Graduate Programs Dropping GRE RequirementJhamy A. SoriaNo ratings yet
- History and Development of Antimicrobial Susceptibility Testing MethodologyDocument7 pagesHistory and Development of Antimicrobial Susceptibility Testing MethodologyTogu NaiposposNo ratings yet
- Microbiology Lab Report AnalysisDocument8 pagesMicrobiology Lab Report AnalysisMythily ChandirasegaranNo ratings yet
- Restriction Enzymes PDFDocument7 pagesRestriction Enzymes PDFmanoj_rkl_07No ratings yet
- Usfda Pharma Plants IndiaDocument4 pagesUsfda Pharma Plants IndiaTaherNo ratings yet
- Genetic Codes With No Dedicated Stop Codon Context Dependent Translation TerminationDocument13 pagesGenetic Codes With No Dedicated Stop Codon Context Dependent Translation TerminationAarcamNo ratings yet
- Genetically Modified Foods and Social ConcernsDocument8 pagesGenetically Modified Foods and Social ConcernsLeika GonzalesNo ratings yet
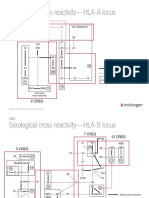
- Serological cross-reactivity-HLA-A Locus: 1 CregDocument5 pagesSerological cross-reactivity-HLA-A Locus: 1 CregGeorgia MarcussoNo ratings yet
- Internship Report: Name: Nabeel Mohammed Iitm - 5 Semester Biological Engineering BE12B017Document49 pagesInternship Report: Name: Nabeel Mohammed Iitm - 5 Semester Biological Engineering BE12B017Nabeel MohammedNo ratings yet
- NABL 112 Effective From 01.06.2019 PDFDocument102 pagesNABL 112 Effective From 01.06.2019 PDFSp PpvNo ratings yet
- Aeration and AgitationDocument5 pagesAeration and Agitationdadang71No ratings yet
- Structure and Organization of Human GenomeDocument18 pagesStructure and Organization of Human GenomeMudasir AyubNo ratings yet
- Melbourne University - Parkville Campus MapDocument1 pageMelbourne University - Parkville Campus MapЯyuTenNo ratings yet
- Genomic Library - Hongming LamDocument72 pagesGenomic Library - Hongming LamYixuan ZhuNo ratings yet
- Time 120Document3 pagesTime 120ardhra pNo ratings yet
- Agricultural Biotechnology Background and Recent Issues SummaryDocument44 pagesAgricultural Biotechnology Background and Recent Issues SummaryNathiyaNo ratings yet