You might also like
- Frozen Section Pathology: Diagnostic ChallengesFrom EverandFrozen Section Pathology: Diagnostic ChallengesAlain C. BorczukNo ratings yet
- Patient-Initiated Device Removal in Intensive Care Units - A National Prevalence StudyDocument7 pagesPatient-Initiated Device Removal in Intensive Care Units - A National Prevalence StudyJim LinNo ratings yet
- 3423 Emergency Tracheal Intubations at A University HospitalDocument7 pages3423 Emergency Tracheal Intubations at A University HospitalAnaNo ratings yet
- Jurnal VentilasiDocument10 pagesJurnal Ventilasiarif21492No ratings yet
- Daily Interruption of Sedation in Patients Receiving Mechanical VentilationDocument10 pagesDaily Interruption of Sedation in Patients Receiving Mechanical VentilationEryll Jean SamotNo ratings yet
- Is It Safe To Discharge Intussusception Patients After Successful Hydrostatic Reduction?Document5 pagesIs It Safe To Discharge Intussusception Patients After Successful Hydrostatic Reduction?DaGiTrVel'zNo ratings yet
- Ektub 1Document7 pagesEktub 1Muhamad ArwaniNo ratings yet
- 10 1097@CCM 0b013e31818b35f2Document7 pages10 1097@CCM 0b013e31818b35f2omarihuanoNo ratings yet
- Predictor de ExtubacionDocument10 pagesPredictor de Extubacionmomis_92No ratings yet
- 325 WHO Surgical Safety ChecklistDocument8 pages325 WHO Surgical Safety ChecklistAlfie YannurNo ratings yet
- Geriatric Nursing: Canan Karadas, MSC, Leyla Ozdemir, RN, PHDDocument6 pagesGeriatric Nursing: Canan Karadas, MSC, Leyla Ozdemir, RN, PHDCharah IC NuRseNo ratings yet
- Recent Key PublicationsDocument3 pagesRecent Key PublicationserdNo ratings yet
- Early Identification of Patients at Risk For Difficult Intubation in The Intensive Care UnitDocument9 pagesEarly Identification of Patients at Risk For Difficult Intubation in The Intensive Care UnitAlfredoNoriegaPonceeNo ratings yet
- 13-2 Collated 3 (3) - 149-155Document7 pages13-2 Collated 3 (3) - 149-155Inas AzharNo ratings yet
- Clinical Trials and Regulatory Science in CardiologyDocument6 pagesClinical Trials and Regulatory Science in Cardiologydianaerlita97No ratings yet
- Patient Safety During Sedation by Anesthesia ProfeDocument8 pagesPatient Safety During Sedation by Anesthesia ProfeIsmar MorenoNo ratings yet
- Evidence of Self-Directed Learning: 1. Reflection On Ectopic Pregnancy RetrievedDocument3 pagesEvidence of Self-Directed Learning: 1. Reflection On Ectopic Pregnancy RetrievedJasha MaeNo ratings yet
- Artigo - INTUBAÇÃO - Cabeceira ElevadaDocument7 pagesArtigo - INTUBAÇÃO - Cabeceira Elevadatt6jj7pgpxNo ratings yet
- Original Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization PracticesDocument12 pagesOriginal Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization Practicesandi kurniawanNo ratings yet
- Management of Intra-Abdominally Translocated Contraceptive Devices, Is Surgery The Only Way To Treat This Problem?Document8 pagesManagement of Intra-Abdominally Translocated Contraceptive Devices, Is Surgery The Only Way To Treat This Problem?Rezky amalia basirNo ratings yet
- The Extent of Knowledge and Participation of The Staff Nurses On The Visual Infusion Phlebitis Program of Saint Anthony College HospitalDocument89 pagesThe Extent of Knowledge and Participation of The Staff Nurses On The Visual Infusion Phlebitis Program of Saint Anthony College HospitalWinj BudayNo ratings yet
- The Clinical Impact of Ventilator-Associated Events - Zhu2015Document8 pagesThe Clinical Impact of Ventilator-Associated Events - Zhu2015Maxi BoniniNo ratings yet
- tmp8342 TMPDocument7 pagestmp8342 TMPFrontiersNo ratings yet
- Achieving Sustainability in Reducing Unplanned Extubations in PICUDocument7 pagesAchieving Sustainability in Reducing Unplanned Extubations in PICUKevin Bazán TorrealvaNo ratings yet
- Extubacion British 2010Document4 pagesExtubacion British 2010fciccioliNo ratings yet
- Urinary 1Document7 pagesUrinary 1Yuni AstutiNo ratings yet
- Effect of Implementation of A Surgical Safety Checklist On Perioperative and Postoperative Complications at An Academic Institution in North AmericaDocument14 pagesEffect of Implementation of A Surgical Safety Checklist On Perioperative and Postoperative Complications at An Academic Institution in North AmericaMuhammad BasharatullahNo ratings yet
- Jurnal Kritis ICU Bundle Vap PneumoniaDocument6 pagesJurnal Kritis ICU Bundle Vap PneumoniaAdzkia PintaNo ratings yet
- 1 s2.0 S1053077022009168 MainDocument8 pages1 s2.0 S1053077022009168 MainOttofianus Alvedo Hewick KalangiNo ratings yet
- Risk Factors For Ventilator-Associated Events - Liu 2019Document6 pagesRisk Factors For Ventilator-Associated Events - Liu 2019Maxi BoniniNo ratings yet
- Shaffer2017-Tutku MacBook ProDocument6 pagesShaffer2017-Tutku MacBook ProMEKSELINA KALENDERNo ratings yet
- CJRT 2019 011Document8 pagesCJRT 2019 011Siti HumairahNo ratings yet
- Assessment and Management of Preoperative AnxietyDocument6 pagesAssessment and Management of Preoperative AnxietyFiorel Loves EveryoneNo ratings yet
- Aj Infection Control 2011 Vestimenta de Enf y Medicos Como Posible Fuente de Infeccion NosocomialDocument5 pagesAj Infection Control 2011 Vestimenta de Enf y Medicos Como Posible Fuente de Infeccion NosocomialJuanNo ratings yet
- ICHEDocument6 pagesICHEoliviayusandaNo ratings yet
- Penetalaksanaan Syok (Rizki Devita Roshella)Document9 pagesPenetalaksanaan Syok (Rizki Devita Roshella)rizki devta roshellaiNo ratings yet
- Mobilisasi MV ICUDocument12 pagesMobilisasi MV ICUArmi ZakaNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka Annexure - Ii Proforma For Registration of Subject For DissertationDocument17 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka Annexure - Ii Proforma For Registration of Subject For DissertationyashramawatNo ratings yet
- Robert K. Fitzgerald - Multicenter Analysis of The Factors Associated With Unplanned Extubation in The PICUDocument7 pagesRobert K. Fitzgerald - Multicenter Analysis of The Factors Associated With Unplanned Extubation in The PICUKevin Bazán TorrealvaNo ratings yet
- Zhou 2011Document7 pagesZhou 2011MARCO ANTONIONo ratings yet
- Medical Versus Surgical Termination of The First Trimester Missed MiscarriageDocument5 pagesMedical Versus Surgical Termination of The First Trimester Missed Miscarriageujjwal souravNo ratings yet
- What Are The Barriers To Mobilizing Intensive Care Patients?Document4 pagesWhat Are The Barriers To Mobilizing Intensive Care Patients?Tote Cifuentes AmigoNo ratings yet
- Australian Critical CareDocument9 pagesAustralian Critical CareLisa MaghfirahNo ratings yet
- Pone 0129434Document15 pagesPone 0129434api-325197812No ratings yet
- Prehospital Airway Management: A Systematic ReviewDocument13 pagesPrehospital Airway Management: A Systematic ReviewmirzaNo ratings yet
- Infection Prevention in The Neurointensive Care Unit: A Systematic ReviewDocument15 pagesInfection Prevention in The Neurointensive Care Unit: A Systematic ReviewDžiugas KrNo ratings yet
- AJA2019 Cspine ExtubationDocument7 pagesAJA2019 Cspine ExtubationSeveNNo ratings yet
- Percutaneous Implantation of An Entirely Intracardiac Leadless PacemakerDocument11 pagesPercutaneous Implantation of An Entirely Intracardiac Leadless PacemakerRaul OrtegaNo ratings yet
- Guia IDSA Prevencion ICVCDocument32 pagesGuia IDSA Prevencion ICVCmaturana61No ratings yet
- Medi 101 E30007Document6 pagesMedi 101 E30007Hadley AuliaNo ratings yet
- Paper Reintubación Variable Sexo y EdadDocument5 pagesPaper Reintubación Variable Sexo y EdadAres Kinesiology TapeNo ratings yet
- Aborto Septico Lanari-USA ICM 2004Document6 pagesAborto Septico Lanari-USA ICM 2004pastorizaariana25No ratings yet
- Rba 0 AheadOfPrint 6036c54fa95395582f07f644Document5 pagesRba 0 AheadOfPrint 6036c54fa95395582f07f644STRMoch Hafizh AlfiansyahNo ratings yet
- Neonatal PneumoniaDocument8 pagesNeonatal PneumoniaAde Gustina SiahaanNo ratings yet
- The Incidence and Severity of Adverse Events Affecting Patients After Discharge From The HospitalDocument14 pagesThe Incidence and Severity of Adverse Events Affecting Patients After Discharge From The Hospitalrobert93No ratings yet
- PHYS THER-2013-Clark-186-96Document13 pagesPHYS THER-2013-Clark-186-96Ratih Dwi LestariNo ratings yet
- Journal Cardiac ArrestDocument6 pagesJournal Cardiac ArrestDavid Fransiskus SimarmataNo ratings yet
- DE LA CRUZ Prevención de Infección Del Sitio Quirúrgico - ArtDocument6 pagesDE LA CRUZ Prevención de Infección Del Sitio Quirúrgico - ArtJOSE FERNANDO DE LA CRUZ SILVANNo ratings yet
- Long-Stay of PICU in SepsisDocument6 pagesLong-Stay of PICU in SepsisSanti IskandarNo ratings yet
- LG RN Ad For WebDocument1 pageLG RN Ad For WebbagsikNo ratings yet
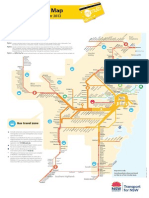
- Mymulti Fare MapDocument1 pageMymulti Fare Maphoneytrap99No ratings yet
- Visit Transportnsw - Info: Description of Routes in This Timetable Route 611Document11 pagesVisit Transportnsw - Info: Description of Routes in This Timetable Route 611bagsikNo ratings yet
- NANDA NursingDocument159 pagesNANDA NursingAijem RyanNo ratings yet
- Approach To Coma SC FinalDocument57 pagesApproach To Coma SC FinalsubhankarNo ratings yet
- Treatment Plan: Case Study #1 "Donald"Document19 pagesTreatment Plan: Case Study #1 "Donald"api-525319529No ratings yet
- Consensus Statement On Brain Death - Malaysia - 2003Document25 pagesConsensus Statement On Brain Death - Malaysia - 2003docpunit100% (1)
- Glasgow Come ScaleDocument11 pagesGlasgow Come ScaleMaria Jose Gonzalez SarangoNo ratings yet
- Hepatic ComaDocument4 pagesHepatic ComaAshraf Abu-ainNo ratings yet
- Convultion-: EndocarditisDocument2 pagesConvultion-: Endocarditisjuanito c garado jrNo ratings yet
- Pradnya E Combine For PDFDocument44 pagesPradnya E Combine For PDFSai PuppalaNo ratings yet
- NCP AlteredDocument3 pagesNCP AlteredShaira TillahNo ratings yet
- A Subdural HematomaDocument2 pagesA Subdural HematomaMohammadAwitNo ratings yet
- Retrospective Characterization of Coma and Stupor in Dogs and Cats Presenting To A Multicenter Out-Of-Hours Service (2012-2015) : 386 AnimalsDocument7 pagesRetrospective Characterization of Coma and Stupor in Dogs and Cats Presenting To A Multicenter Out-Of-Hours Service (2012-2015) : 386 AnimalsLaura Pereira da SilvaNo ratings yet
- Death EssayDocument3 pagesDeath EssayJonathan BoardmanNo ratings yet
- Normal Vital Signs Guidelines For EmsDocument4 pagesNormal Vital Signs Guidelines For EmsJonathan delos ReyesNo ratings yet
- Lab Act 1 - Motor AssessmentDocument6 pagesLab Act 1 - Motor AssessmentZgama AbdulrahmanNo ratings yet
- FCCS Critical Care SheetDocument21 pagesFCCS Critical Care SheetLore Anne Mhae SantosNo ratings yet
- BIND Score PDFDocument1 pageBIND Score PDFSindhumv GowdaNo ratings yet
- Meningitis TBC Lancet PDFDocument11 pagesMeningitis TBC Lancet PDFGustavo MartinezNo ratings yet
- MusculoskeletalDocument36 pagesMusculoskeletalNat Lynne Distor TrondilloNo ratings yet
- Neurologic Emergencies Michael J. Caudell, M.D., FACEPDocument10 pagesNeurologic Emergencies Michael J. Caudell, M.D., FACEPBiswaranjan PadhyNo ratings yet
- Clear My Choice: Not Yet Answered Marked Out of 1.00Document34 pagesClear My Choice: Not Yet Answered Marked Out of 1.00mark OrpillaNo ratings yet
- The One That Got Away ScriptDocument12 pagesThe One That Got Away ScriptMarisa BaterNo ratings yet
- Adult Neurological ExaminationDocument57 pagesAdult Neurological ExaminationSandeep Soni100% (1)
- Cerebellar InfarctionDocument23 pagesCerebellar InfarctionShane LuyNo ratings yet
- Nursing Practice IvDocument24 pagesNursing Practice IvJohn wewNo ratings yet
- Trauma McqsDocument12 pagesTrauma Mcqschanaish6100% (1)
- 15 Item ACLS Drill Answers and RationaleDocument6 pages15 Item ACLS Drill Answers and RationaleAijem RyanNo ratings yet
- Lim Vs ChincoDocument3 pagesLim Vs ChincoAlyanna ChangNo ratings yet
- Coma-Causes, Diagnosis, Treatment and ManagementDocument19 pagesComa-Causes, Diagnosis, Treatment and ManagementHabtamu AdimasuNo ratings yet
- Brain Stem Death: Learning ObjectivesDocument4 pagesBrain Stem Death: Learning ObjectivesFarizNo ratings yet
- Managing - Patients - With - Severe - Traumatic - Brain WITH HIGHLIGHTSDocument8 pagesManaging - Patients - With - Severe - Traumatic - Brain WITH HIGHLIGHTSTre OfficialNo ratings yet
- Neurological ExaminationDocument55 pagesNeurological ExaminationWasemBhatNo ratings yet