You might also like
- Cardiovascular Fluid DynamicsFrom EverandCardiovascular Fluid DynamicsD.H. BergelNo ratings yet
- Gad-7 Questionnaire SpanishDocument86 pagesGad-7 Questionnaire Spanishrowanpurdy100% (1)
- Pulmonary Function TestDocument7 pagesPulmonary Function TestGhada HusseinNo ratings yet
- Pulmonary Function Testing1Document51 pagesPulmonary Function Testing1kusaarNo ratings yet
- Pulmonary Function Test Part 1 PPTDR Mona AllangawiDocument84 pagesPulmonary Function Test Part 1 PPTDR Mona Allangawisachin10dulkarNo ratings yet
- Overview of Mechanical Ventilation Settings, Modes, TroubleshootingDocument24 pagesOverview of Mechanical Ventilation Settings, Modes, TroubleshootingRochim CoolNo ratings yet
- PEEP (Positive-End Expiratory Pressure)Document5 pagesPEEP (Positive-End Expiratory Pressure)Valcrist BalderNo ratings yet
- Dr. Kannan Nair's Guide to Non-Invasive Ventilation Settings and ModesDocument62 pagesDr. Kannan Nair's Guide to Non-Invasive Ventilation Settings and ModesKannan NairNo ratings yet
- Mechanical Ventilation AulaDocument47 pagesMechanical Ventilation Aulaapi-3820606100% (1)
- Pulmonary Rehabilitation PPDocument19 pagesPulmonary Rehabilitation PPnashqonashNo ratings yet
- Conquering the Ventilation JungleDocument69 pagesConquering the Ventilation Jungledr_nkhan3415No ratings yet
- Magic of TouchDocument28 pagesMagic of TouchkurniawatiNo ratings yet
- Respiratory Function TestDocument7 pagesRespiratory Function TestMarivic DianoNo ratings yet
- MKULTRA Briefing Book SummaryDocument396 pagesMKULTRA Briefing Book SummaryTsz Kwan LiaoNo ratings yet
- PepDocument18 pagesPepAdrian DedicNo ratings yet
- Pulmonary Function TestsDocument25 pagesPulmonary Function TestsRaviNo ratings yet
- Pulmonary Rehabilitation Slide PresentationDocument24 pagesPulmonary Rehabilitation Slide Presentationdranoj0070% (1)
- Cystic FibrosisDocument40 pagesCystic FibrosisMoonmoon SinhaNo ratings yet
- Better Living With COPDDocument108 pagesBetter Living With COPDPrem AnandNo ratings yet
- Graves DseDocument5 pagesGraves DseHester Marie SimpiaNo ratings yet
- Pulmonary Function TestsDocument35 pagesPulmonary Function Testsnirilib100% (4)
- Superior Vena Cava Syndrome WewwDocument8 pagesSuperior Vena Cava Syndrome WewwIgnatius Yuwanda ChrissanderNo ratings yet
- Intestinal DisordersDocument11 pagesIntestinal DisorderspulmonologistNo ratings yet
- Acute Respiratory Distress SyndromeDocument77 pagesAcute Respiratory Distress SyndromeAnnisa Dyah ChairiniNo ratings yet
- Basic Respiratory Mechanics: Ventilation, Diffusion, and Gas ExchangeDocument36 pagesBasic Respiratory Mechanics: Ventilation, Diffusion, and Gas ExchangeRizqi Luqmanul HakimNo ratings yet
- Rheumatic Heart Disease: Causes, Symptoms and PathologyDocument23 pagesRheumatic Heart Disease: Causes, Symptoms and PathologymelaikoNo ratings yet
- Thorax and The LungsDocument30 pagesThorax and The Lungschifunndo charles100% (1)
- Pulmonary SystemDocument75 pagesPulmonary Systemangeles_robert_71No ratings yet
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- Rsexm 170207141549Document72 pagesRsexm 170207141549gpete321No ratings yet
- Hahn, R. 1995. Sickness and Healing - An Anthropological Perspective. Chap 4 - The Role of Society and Culture in Sickness and HealingDocument24 pagesHahn, R. 1995. Sickness and Healing - An Anthropological Perspective. Chap 4 - The Role of Society and Culture in Sickness and HealingJenny Gill67% (3)
- Diagnostic Thoracoscopy (VATS) in Lung CancerDocument18 pagesDiagnostic Thoracoscopy (VATS) in Lung CancerlmdarlongNo ratings yet
- Pulmonary Function TestsDocument20 pagesPulmonary Function TestsMohamedSalah100% (2)
- Pulmonary Function Test and Sputum CultureDocument14 pagesPulmonary Function Test and Sputum CultureGeorgea Beleni S. AbinesNo ratings yet
- Levels of Prevention ModelDocument3 pagesLevels of Prevention ModelSachin Konkani67% (3)
- Spiro Me Try Cheat Sheet 09Document2 pagesSpiro Me Try Cheat Sheet 09Yudha Perwira PutraNo ratings yet
- Pulmonary Function Tests (PFT)Document30 pagesPulmonary Function Tests (PFT)براءة أحمد السلاماتNo ratings yet
- Lung AuscultationDocument62 pagesLung AuscultationOlea CroitorNo ratings yet
- Aerosoltherapy Nebu 120503115712 Phpapp01Document65 pagesAerosoltherapy Nebu 120503115712 Phpapp01Aan Ika SugathotNo ratings yet
- NEJM 2014 Fundamentals of Lung AuscultationDocument7 pagesNEJM 2014 Fundamentals of Lung AuscultationFelipe CeaNo ratings yet
- 33 Airway ManagementDocument19 pages33 Airway ManagementTiffany Helmes100% (2)
- AerosolsDocument9 pagesAerosolsTubaNo ratings yet
- Mechanical Ventilation Modes, Settings and CareDocument40 pagesMechanical Ventilation Modes, Settings and CarePratik SahooNo ratings yet
- Airway Clearance Physiology Pharmacology Techniques and Practice PDFDocument5 pagesAirway Clearance Physiology Pharmacology Techniques and Practice PDFPaoly PalmaNo ratings yet
- Intermittent Positive Pressure BreathingDocument12 pagesIntermittent Positive Pressure BreathingHitesh RohitNo ratings yet
- Postural, DrainageDocument7 pagesPostural, DrainageJames ThompsonNo ratings yet
- Bronchial Hygiene Therapy Lecture CHP 40Document18 pagesBronchial Hygiene Therapy Lecture CHP 40Ion FloreaNo ratings yet
- BRONCHIECTASISDocument36 pagesBRONCHIECTASISVince Peliño De MesaNo ratings yet
- Mechanical Ventilation and Intracranial PressureDocument30 pagesMechanical Ventilation and Intracranial PressureFlavius AnghelNo ratings yet
- ECG Practical Notes TypesDocument2 pagesECG Practical Notes TypesRich ColeNo ratings yet
- Lung Expansion RevisionDocument89 pagesLung Expansion RevisionPatrick RoqueNo ratings yet
- Pulmonary Function TestsDocument38 pagesPulmonary Function TestsMohamedSalahNo ratings yet
- Respiratory EmergenciesDocument34 pagesRespiratory EmergenciesRoshana MallawaarachchiNo ratings yet
- The Management of Acute Respiratory Distress SyndromeDocument48 pagesThe Management of Acute Respiratory Distress SyndromeLauraAlvarezMulettNo ratings yet
- Basic Principles of Pediatric Mechanical VentilationDocument39 pagesBasic Principles of Pediatric Mechanical VentilationNav KovNo ratings yet
- Essential Concepts for Airway ManagementDocument42 pagesEssential Concepts for Airway Managementkader abdiNo ratings yet
- Elasticity, Surfactant, Surface Tension and Compliance: Prof - Hafeezul HassanDocument26 pagesElasticity, Surfactant, Surface Tension and Compliance: Prof - Hafeezul HassanDr. Zaheer AliNo ratings yet
- An Approach To A Patient With BreathlessnessDocument35 pagesAn Approach To A Patient With Breathlessnessgl tousifNo ratings yet
- COPD Acute Management ABCDEDocument11 pagesCOPD Acute Management ABCDESSNo ratings yet
- Chapter 19 PULMONARY FUNCTION TESTINGDocument13 pagesChapter 19 PULMONARY FUNCTION TESTINGZahra Margrette Schuck0% (1)
- Extubation CriteriaDocument17 pagesExtubation CriteriaOliver TabagNo ratings yet
- Mechanical Ventilation TherapyDocument17 pagesMechanical Ventilation TherapyFaizal FlNo ratings yet
- Respiratory DrugsDocument20 pagesRespiratory DrugsMelanesiaNo ratings yet
- One Lung VentilationDocument24 pagesOne Lung Ventilationapi-254759511No ratings yet
- Abdominal IncisionDocument4 pagesAbdominal IncisionMohit KumarNo ratings yet
- X Thorax BeoordelenDocument135 pagesX Thorax BeoordelenmtescasuraNo ratings yet
- Pulmonary Function TestDocument34 pagesPulmonary Function TestmukeshmscNo ratings yet
- 66 Neonatal Resuscitation Show Notes 1Document3 pages66 Neonatal Resuscitation Show Notes 1Rabbani IcksanNo ratings yet
- Burn ppt shashi: Key points on burn managementDocument4 pagesBurn ppt shashi: Key points on burn managementSachin KonkaniNo ratings yet
- TBDocument11 pagesTBSachin KonkaniNo ratings yet
- Burns Management PDFDocument7 pagesBurns Management PDFRoh Bungaria N Garingging100% (1)
- HerniaDocument3 pagesHerniaSachin KonkaniNo ratings yet
- Sigmund Freud's TheoryDocument22 pagesSigmund Freud's TheoryGil Mark B TOmas100% (2)
- 81 - Review of The Clinical Efficacy of Traumeel PDFDocument14 pages81 - Review of The Clinical Efficacy of Traumeel PDFmdkkavathekarNo ratings yet
- The Crashing Ventilated Patient Algorthm (Jairo I. Santanilla, ACEP, 2011)Document1 pageThe Crashing Ventilated Patient Algorthm (Jairo I. Santanilla, ACEP, 2011)PkernNo ratings yet
- Essential medicines certificateDocument2 pagesEssential medicines certificateAnji KaringuNo ratings yet
- Pennsylvania Report On Adult Use Recreational MarijuanaDocument89 pagesPennsylvania Report On Adult Use Recreational MarijuanaMarijuana MomentNo ratings yet
- Proquest Research Library Health and MedicineDocument1,290 pagesProquest Research Library Health and MedicineIng Mauricio SabogalNo ratings yet
- Bone: Cystic & Neoplastic LesionsDocument83 pagesBone: Cystic & Neoplastic LesionsPuspita PrihatiniNo ratings yet
- Pfizer Et. Al. v. Intas Pharmaceuticals Et. Al.Document15 pagesPfizer Et. Al. v. Intas Pharmaceuticals Et. Al.PriorSmartNo ratings yet
- JVPDocument5 pagesJVPYhr YhNo ratings yet
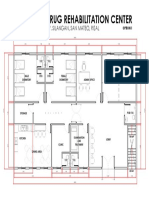
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNo ratings yet
- Transitioning Anticoagulants 2016Document4 pagesTransitioning Anticoagulants 2016S_XangaiNo ratings yet
- Dithranol (Dithocream) Treatment For Alopecia Areata Mar 19Document5 pagesDithranol (Dithocream) Treatment For Alopecia Areata Mar 19Pakeeza FatimaNo ratings yet
- Basic Splinting TechniquesDocument5 pagesBasic Splinting TechniquesAdy KimNo ratings yet
- Methods of Gaining Space 2012 - 2Document3 pagesMethods of Gaining Space 2012 - 2Ahmad KhaledNo ratings yet
- DPT Doctor of Physiotherapy Program at Abu Zafar InstituteDocument44 pagesDPT Doctor of Physiotherapy Program at Abu Zafar InstituteAbdul basit KaleemNo ratings yet
- Nurse Practitioner VS Physical TherapistsDocument5 pagesNurse Practitioner VS Physical Therapistspdet1No ratings yet
- Essesntial Drug List PakistanDocument46 pagesEssesntial Drug List Pakistanirfanmajeed1987No ratings yet
- Peds PresentationDocument31 pagesPeds Presentationapi-247218432No ratings yet
- Assignment 3 4 Relapse Prevention Paper Brian MannDocument8 pagesAssignment 3 4 Relapse Prevention Paper Brian Mannapi-301673059No ratings yet
- Atlas de Oncologia Clinica PDFDocument512 pagesAtlas de Oncologia Clinica PDFAlfonso Carlos Gutierrez MartinezNo ratings yet
- A Wee-Bit of Philippine Indigenous TherapiesDocument8 pagesA Wee-Bit of Philippine Indigenous TherapiesEunice100% (6)
- Sensory Deprivation and Loss-4Document32 pagesSensory Deprivation and Loss-4Scott Daniel Phillips100% (1)
- Community Building ProcessDocument17 pagesCommunity Building ProcessKarolina HutagalungNo ratings yet