You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- r09 Distributed DatabasesDocument1 pager09 Distributed Databasesgangadhar5816No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- 5010 837PDocument44 pages5010 837Pgangadhar5816No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Basics of SCSI Fourth EditionDocument59 pagesBasics of SCSI Fourth EditionDušanka LapčićNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 837 Health Care Claim Payment Advice Procedure Code Bundling UnbundlingDocument9 pages837 Health Care Claim Payment Advice Procedure Code Bundling UnbundlingvalmikigangadharNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- CachesDocument62 pagesCachesgangadhar5816No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Langkawi - AcommodationDocument8 pagesLangkawi - AcommodationSaidahMohamedNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Data Flow DiagramDocument7 pagesData Flow Diagramcalliezx13No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Sec CoinDocument102 pagesSec CoinZerohedgeNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Mr. Puneeth Kumar D's bank account statement from Dec 2019 to Jun 2020Document4 pagesMr. Puneeth Kumar D's bank account statement from Dec 2019 to Jun 2020Puneeth KumarNo ratings yet
- Retailing Chapter 4Document7 pagesRetailing Chapter 4Richard AquinoNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Fact Orders Tec Stored A To S 2022Document2,364 pagesFact Orders Tec Stored A To S 2022Mikel SUAREZ BARREIRONo ratings yet
- Wholesale Real Estate Purchase Agreement PSA1Document1 pageWholesale Real Estate Purchase Agreement PSA1Charles Gonzales100% (6)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Modicare Distribution Point Policies and Procedures GuideDocument53 pagesModicare Distribution Point Policies and Procedures Guideisometric_view78% (9)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- FTPartnersResearch InsuranceTechnologyTrendsDocument248 pagesFTPartnersResearch InsuranceTechnologyTrendsmeNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
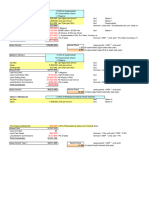
- F3X26-TB Industrial 4G LTE RouterDocument6 pagesF3X26-TB Industrial 4G LTE RouterBernardoNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Alpha Prefix List Reg-PremDocument3 pagesAlpha Prefix List Reg-Premseattlecarol0% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Leslie Turner CH 8Document59 pagesLeslie Turner CH 8AYI FADILLAHNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- 7Ps of Marketing Mix of ICICI BankDocument8 pages7Ps of Marketing Mix of ICICI Bankgktest4321100% (3)
- Inz 1183Document2 pagesInz 1183nad.liveNo ratings yet
- Unit 2 - BilpDocument14 pagesUnit 2 - BilpYashika GuptaNo ratings yet
- D2.2 2300Mhz Role and Values in Network Performance and 4G 5G Spectrum AnalysisDocument20 pagesD2.2 2300Mhz Role and Values in Network Performance and 4G 5G Spectrum Analysishaipm1979No ratings yet
- Consumer Finance GuideDocument28 pagesConsumer Finance GuiderajatNo ratings yet
- E Bill ReceiptDocument1 pageE Bill Receiptshivg2213No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- PNBDocument6 pagesPNBCristine Damirez TadleNo ratings yet
- Indian Economy and Service SectorDocument30 pagesIndian Economy and Service Sectorpavani pydiNo ratings yet
- CV: Tengku Bobby LesmanaDocument8 pagesCV: Tengku Bobby LesmanaBobbyNo ratings yet
- Rapides Parish Sheriff's Office Audit ReportDocument55 pagesRapides Parish Sheriff's Office Audit ReportThe Town TalkNo ratings yet
- Guidance Installation SDA AntennaDocument22 pagesGuidance Installation SDA AntennaYorico Bhaskara ManoppoNo ratings yet
- WWW - Bankofindia.co - in UserFiles File DebitCumATMCardApplicationDocument1 pageWWW - Bankofindia.co - in UserFiles File DebitCumATMCardApplicationSiddharth ShanbhogueNo ratings yet
- Computer Networks Lesson Plan Materials Computer Networks Lesson Plan MaterialsDocument6 pagesComputer Networks Lesson Plan Materials Computer Networks Lesson Plan MaterialsAldrin Canicula CompetenteNo ratings yet
- Natureview Farm Case Calculations Pre-Class SpreadsheetDocument12 pagesNatureview Farm Case Calculations Pre-Class Spreadsheet1010478907No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Hulo Integrated National High School Contact DetailsDocument36 pagesHulo Integrated National High School Contact DetailsHellen.DeaNo ratings yet
- HLB Receipt-2023-05-17 2Document3 pagesHLB Receipt-2023-05-17 2v6wxcvjmvgNo ratings yet
- Toll Free MatrixDocument1 pageToll Free MatrixTAPAN KUMAR BEHERANo ratings yet
- Diameter Charging EnablingDocument110 pagesDiameter Charging EnablingJahan ZebNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)