You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Westminster Academy, Islamabad: Physics (0625) Topic Test:Sound WavesDocument5 pagesWestminster Academy, Islamabad: Physics (0625) Topic Test:Sound Wavessaimee77No ratings yet
- B 2Document12 pagesB 2Mohamed Sayed Abdel GaffarNo ratings yet
- Sybsc Physics Practical Usphp3Document3 pagesSybsc Physics Practical Usphp3Ujjwala GokheNo ratings yet
- Business Analyst TrainingDocument3 pagesBusiness Analyst TrainingMuniswamaiah Mohan100% (1)
- 384 TungaloyDocument32 pages384 Tungaloyp.designNo ratings yet
- KujiDocument17 pagesKujiGorumbha Dhan Nirmal Singh100% (2)
- Report On The Quantitative Techniques in BusinessDocument10 pagesReport On The Quantitative Techniques in BusinessBaron FrancisNo ratings yet
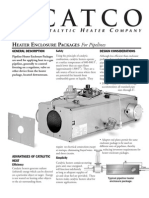
- Calentador Catalitico de TuberíasDocument2 pagesCalentador Catalitico de TuberíasDavid RomeroNo ratings yet
- Science8 Q2 Module3 (Week6)Document30 pagesScience8 Q2 Module3 (Week6)Mary Grace Lemon100% (1)
- Basic Hydraulic SystemsDocument128 pagesBasic Hydraulic Systemsbeau04297% (35)
- Martillo Hyd Atlas Copco SB 150Document12 pagesMartillo Hyd Atlas Copco SB 150Nain murilloNo ratings yet
- Medical Oxygen Cylinder Filling System User ManualDocument57 pagesMedical Oxygen Cylinder Filling System User ManualAldo Tolaba QuirogaNo ratings yet
- Problem Set 1 CirclesDocument2 pagesProblem Set 1 Circlesapi-339611548100% (1)
- AP Calculus BC Study GuideDocument4 pagesAP Calculus BC Study GuideHarshil SahaiNo ratings yet
- Time Signature - WikipediaDocument17 pagesTime Signature - WikipediaDiana GhiusNo ratings yet
- Activity No. 5 Capacitive Circuit ObjectivesDocument4 pagesActivity No. 5 Capacitive Circuit ObjectivesJohn Paul BaquiranNo ratings yet
- Presentation On Power Grid InertiaDocument47 pagesPresentation On Power Grid InertiajorjijonNo ratings yet
- Tutorial - Lecture 3 SolutionsDocument10 pagesTutorial - Lecture 3 SolutionsBastián Olfos MárquezNo ratings yet
- Arm Assembly Language ProgrammingDocument170 pagesArm Assembly Language ProgrammingAnup Kumar Yadav100% (4)
- Splunk Skills Assessment-UpdatedDocument14 pagesSplunk Skills Assessment-Updatedtsegay.csNo ratings yet
- Types of VerbDocument4 pagesTypes of VerbFaisal MalikNo ratings yet
- Measurement of SubstructureDocument24 pagesMeasurement of SubstructureAamaniVeeranam80% (10)
- Week 10 TelecommunicationsDocument7 pagesWeek 10 TelecommunicationsGuido MartinezNo ratings yet
- QR Code Attendance Monitoring SystemDocument6 pagesQR Code Attendance Monitoring Systemjenny adlaoNo ratings yet
- POWER GENERATION FROM OCEAN WAVESDocument14 pagesPOWER GENERATION FROM OCEAN WAVESChersey DoctorNo ratings yet
- Woodward MFR 13Document91 pagesWoodward MFR 13OryaNo ratings yet
- Design of Rigid Pavement CC Road With M30Document2 pagesDesign of Rigid Pavement CC Road With M30Yedla Neelakanteshwar100% (3)
- Water Pinch PresentationDocument14 pagesWater Pinch PresentationDafiMaboNo ratings yet
- Test 2Document16 pagesTest 2edwardNo ratings yet
- Department of Computer Engineering Academic Year 2020-21 Class: SE Computer & IT Subject: 22226 PCI (Programming in C) MCQ Unit 1: Program Logic Development MCQ Question Bank With AnswersDocument8 pagesDepartment of Computer Engineering Academic Year 2020-21 Class: SE Computer & IT Subject: 22226 PCI (Programming in C) MCQ Unit 1: Program Logic Development MCQ Question Bank With AnswersVooovoNo ratings yet