You might also like
- Microf Il Traci OnDocument15 pagesMicrof Il Traci OnCdjuan GnNo ratings yet
- Margenes RestaurativosDocument18 pagesMargenes RestaurativosCdjuan GnNo ratings yet
- Microfiltracion en CarillasDocument6 pagesMicrofiltracion en CarillasCdjuan GnNo ratings yet
- Microfiltracion en CarillasDocument6 pagesMicrofiltracion en CarillasCdjuan GnNo ratings yet
- Early Bone Graft ResortionDocument10 pagesEarly Bone Graft ResortionCdjuan GnNo ratings yet
- Microf Il Traci OnDocument15 pagesMicrof Il Traci OnCdjuan GnNo ratings yet
- Margenes RestaurativosDocument18 pagesMargenes RestaurativosCdjuan GnNo ratings yet
- Eficacia Del Cone Beam para La calidAD OseaDocument7 pagesEficacia Del Cone Beam para La calidAD OseaCdjuan GnNo ratings yet
- Hay Asociacion Entre Calidad DiametroDocument26 pagesHay Asociacion Entre Calidad DiametroCdjuan GnNo ratings yet
- 10 Manadamientos en ImplantologiaDocument2 pages10 Manadamientos en ImplantologiaCdjuan GnNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Calcul BADocument15 pagesCalcul BAHanane BenGamraNo ratings yet
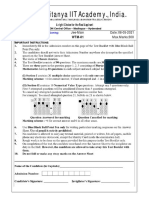
- 08-05-2021 JR - Super60 ActP (In Coming) Jee-Main WTM-01 Question PaperDocument14 pages08-05-2021 JR - Super60 ActP (In Coming) Jee-Main WTM-01 Question Paperpurandar puneetNo ratings yet
- Home Study Report of Resident Indian Parent: Name of The Social WorkerDocument4 pagesHome Study Report of Resident Indian Parent: Name of The Social WorkerVmksNo ratings yet
- Fire & Gas Design BasisDocument2 pagesFire & Gas Design BasisAdil MominNo ratings yet
- Official Game GuideDocument30 pagesOfficial Game GuideHhfugNo ratings yet
- Lappasieugd - 01 12 2022 - 31 12 2022Document224 pagesLappasieugd - 01 12 2022 - 31 12 2022Sri AriatiNo ratings yet
- Iesc101 PDFDocument13 pagesIesc101 PDFBhaskar Sharma0% (1)
- TVL ICT IllustrationNCII Q1Module2Document12 pagesTVL ICT IllustrationNCII Q1Module2Kimberly Trocio Kim100% (1)
- The Earths Internal HeatDocument39 pagesThe Earths Internal Heatkaynechologallardo02No ratings yet
- Soap Making: Borax (NaDocument15 pagesSoap Making: Borax (Naa aNo ratings yet
- Pastillas DelightDocument12 pagesPastillas DelightBryan DutchaNo ratings yet
- Defined Contribution PlanDocument12 pagesDefined Contribution Planrap rapadasNo ratings yet
- Motor Doosan DV11Document220 pagesMotor Doosan DV11David Catari100% (4)
- JMPR 2010 ContentsDocument55 pagesJMPR 2010 ContentsTÙNGNo ratings yet
- Best WiFi Adapter For Kali Linux - Monitor Mode & Packet InjectionDocument14 pagesBest WiFi Adapter For Kali Linux - Monitor Mode & Packet InjectionKoushikNo ratings yet
- ECD KEBVF5 Installation ManualDocument32 pagesECD KEBVF5 Installation Manualashish gautamNo ratings yet
- PKL Geri RevDocument3 pagesPKL Geri RevKurniati NiaNo ratings yet
- Data SheetDocument15 pagesData SheetLucian Sorin BortosuNo ratings yet
- Higuey, Dom Rep Mdpc/Puj: .Eff.23.MayDocument5 pagesHiguey, Dom Rep Mdpc/Puj: .Eff.23.MayVanessa Yumayusa0% (1)
- ABS and Air Conditioner Wiring DiagramDocument207 pagesABS and Air Conditioner Wiring Diagramservice_00783% (30)
- PP Ceylon Graphite Corp February 2023Document16 pagesPP Ceylon Graphite Corp February 2023Siddhant DhallNo ratings yet
- The Benefit of Power Posing Before A High-Stakes Social EvaluationDocument20 pagesThe Benefit of Power Posing Before A High-Stakes Social EvaluationpaolaNo ratings yet
- Basseri TribeDocument3 pagesBasseri TribeMaddah HussainNo ratings yet
- Postnatal Care, Complaints & AbnormalitiesDocument38 pagesPostnatal Care, Complaints & AbnormalitiesBernice GyapongNo ratings yet
- Glaus Corp. inventory note amortization adjusting entryDocument5 pagesGlaus Corp. inventory note amortization adjusting entryPatrick HarponNo ratings yet
- Sara Salon and SpaDocument4 pagesSara Salon and Spasania zehraNo ratings yet
- Masagana High School: Module 4: Planning For Continuing Professional Development and Lac PlanningDocument6 pagesMasagana High School: Module 4: Planning For Continuing Professional Development and Lac PlanningjhonaNo ratings yet
- Energy Certification of Buildings and Nearly Zero-Energy BuildingsDocument70 pagesEnergy Certification of Buildings and Nearly Zero-Energy BuildingsOgnjen BobicicNo ratings yet
- Trilead bis(carbonate) dihydroxide identified as SVHC due to reproductive toxicityDocument7 pagesTrilead bis(carbonate) dihydroxide identified as SVHC due to reproductive toxicityCekinNo ratings yet
- Pub - New Directions in Progressive Relaxation TrainingDocument176 pagesPub - New Directions in Progressive Relaxation TrainingRafael Bagus100% (1)